

Preferences of husbands and wives for outcomes of prostate cancer screening and treatment
- PMID: 15061743
- PMCID: PMC1492196
- DOI: 10.1111/j.1525-1497.2004.30046.x
Preferences of husbands and wives for outcomes of prostate cancer screening and treatment
Abstract
Objective: To explore the preferences of male primary care patients and their spouses for the outcomes of prostate cancer screening and treatment, and quality of life with metastatic prostate cancer.
Design: Cross-sectional design.
Setting: Primary care clinics in Galveston County, Texas.
Patients: One hundred sixty-eight couples in which the husband was a primary care patient and a candidate for prostate cancer screening.
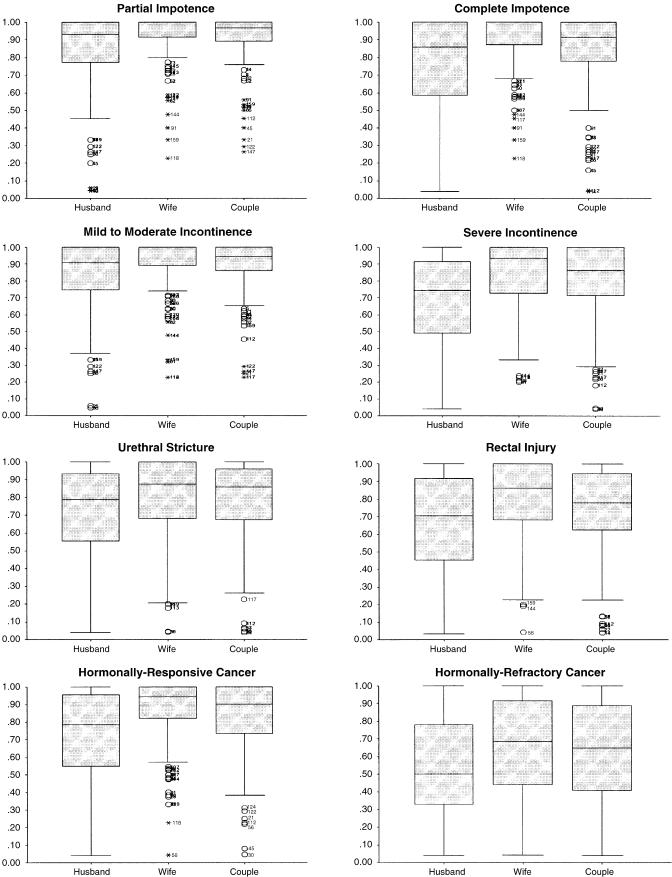
Measurements and main results: Preferences were measured as utilities for treatment outcomes and quality of life with metastatic disease by the time trade-off method for the husband and the wife individually and then conjointly for the couple. For each health state considered, husbands associated lower utilities for the health states than did their wives. Couples' utilities fell between those of husbands and wives (all comparisons were significant at P <.01). For partial and complete impotence and mild-to-moderate incontinence, the median utility value for the wives was 1.0, indicating that most wives did not associate disutility with their husbands having to experience these treatment complications.
Conclusions: Male primary care patients who are candidates for prostate cancer screening evaluate the outcomes of prostate cancer treatment and life with advanced prostate cancer as being far worse than do their wives. Because the choice between quantity and quality of life is a highly individualistic one, both the patient and his partner should be involved in making decisions about prostate cancer screening. J
Figures
References
-
- American Cancer Society. Cancer Facts & Figures 2002. Atlanta, Ga: 2002.
-
- von Eschenbach A, Ho R, Murphy GP, Cunningham M, Lins N. American Cancer Society Guideline for early detection of prostate cancer: update 1997. CA Cancer J Clin. 1997;47:261–4. - PubMed
-
- American Urological Association. Prostate-specific antigen (PSA) best practice policy. Oncology (Huntingt) 2000;14:267–72. 77–8, 280 passim. - PubMed
-
- Barry MJ, Fleming C, Coley CM, Wasson JH, Fahs MC, Oesterling JE. Should Medicare provide reimbursement for prostate-specific antigen testing for early detection of prostate cancer? Part I: framing the debate. Urology. 1995;46:2–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical