

Dependency of magnetocardiographically determined fetal cardiac time intervals on gestational age, gender and postnatal biometrics in healthy pregnancies
- PMID: 15061871
- PMCID: PMC411040
- DOI: 10.1186/1471-2393-4-6
Dependency of magnetocardiographically determined fetal cardiac time intervals on gestational age, gender and postnatal biometrics in healthy pregnancies
Abstract
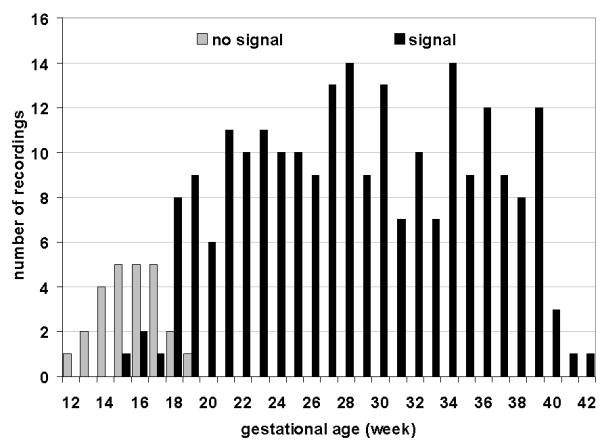
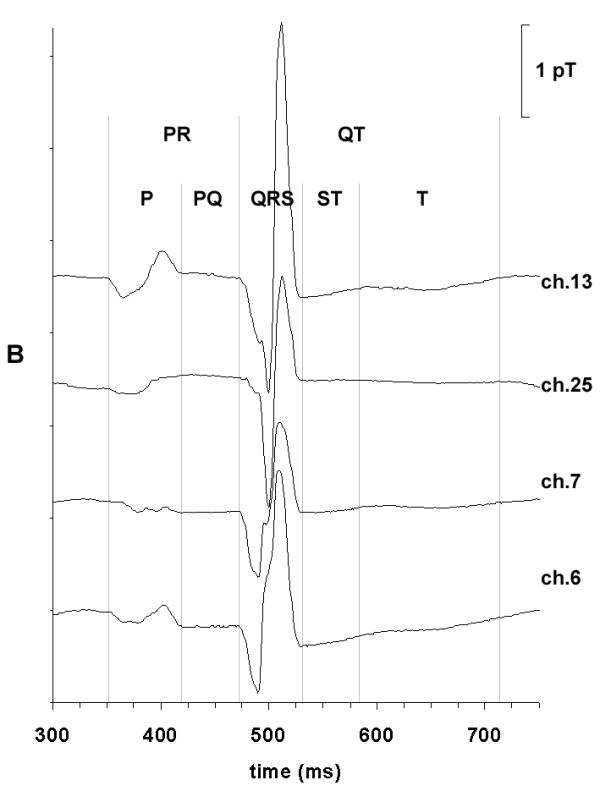
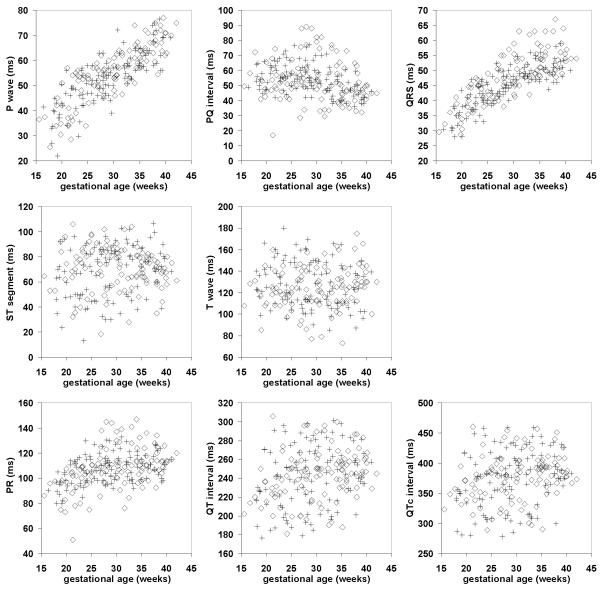
BACKGROUND: Magnetocardiography enables the precise determination of fetal cardiac time intervals (CTI) as early as the second trimester of pregnancy. It has been shown that fetal CTI change in course of gestation. The aim of this work was to investigate the dependency of fetal CTI on gestational age, gender and postnatal biometric data in a substantial sample of subjects during normal pregnancy. METHODS: A total of 230 fetal magnetocardiograms were obtained in 47 healthy fetuses between the 15th and 42nd week of gestation. In each recording, after subtraction of the maternal cardiac artifact and the identification of fetal beats, fetal PQRST courses were signal averaged. On the basis of therein detected wave onsets and ends, the following CTI were determined: P wave, PR interval, PQ interval, QRS complex, ST segment, T wave, QT and QTc interval. Using regression analysis, the dependency of the CTI were examined with respect to gestational age, gender and postnatal biometric data. RESULTS: Atrioventricular conduction and ventricular depolarization times could be determined dependably whereas the T wave was often difficult to detect. Linear and nonlinear regression analysis established strong dependency on age for the P wave and QRS complex (r2 = 0.67, p < 0.001 and r2 = 0.66, p < 0.001) as well as an identifiable trend for the PR and PQ intervals (r2 = 0.21, p < 0.001 and r2 = 0.13, p < 0.001). Gender differences were found only for the QRS complex from the 31st week onward (p < 0.05). The influence on the P wave or QRS complex of biometric data, collected in a subgroup in whom recordings were available within 1 week of birth, did not display statistical significance. CONCLUSION: We conclude that 1) from approximately the 18th week to term, fetal CTI which quantify depolarization times can be reliably determined using magnetocardiography, 2) the P wave and QRS complex duration show a high dependency on age which to a large part reflects fetal growth and 3) fetal gender plays a role in QRS complex duration in the third trimester. Fetal development is thus in part reflected in the CTI and may be useful in the identification of intrauterine growth retardation.
Figures
References
-
- Quinn A, Weir A, Shahani U, Bain R, Maas P, Donaldson G. Antenatal fetal magnetocardiography: a new method for fetal surveillance? Br J Obstet Gynaecol. 1994;101:866–870. - PubMed
-
- Van Leeuwen P, Schüβler M, Bettermann H, Lange S, Hatzmann W. Magnetocardiography for assessment of fetal heart actions. Geburtshilfe Frauenheilkd. 1995;55:642–646. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
