

A trial of automated safety alerts for inpatient digoxin use with computerized physician order entry
- PMID: 15064288
- PMCID: PMC436074
- DOI: 10.1197/jamia.M1500
A trial of automated safety alerts for inpatient digoxin use with computerized physician order entry
Abstract
Objective: Automated clinical decision support (CDS) has shown promise in improving safe medication use. The authors performed a trial of CDS, given both during computerized physician order entry (CPOE) and in response to new laboratory results, comparing the time courses of clinician behaviors related to digoxin use before and after implementation of the alerts.
Design: Alerts were implemented to notify of the potential risk from low electrolyte concentrations or unknown digoxin or electrolyte concentrations during CPOE. Alerts were also generated in response to newly reported hypokalemia and hypomagnesemia in patients given digoxin.
Measurements: Clinician responses to the alerts for six months were compared with responses to similar situations for six months prior to implementation.
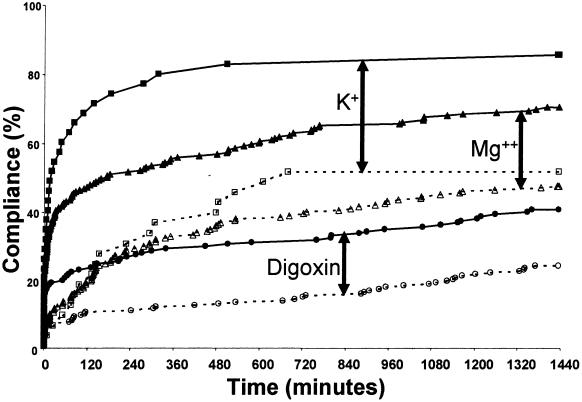
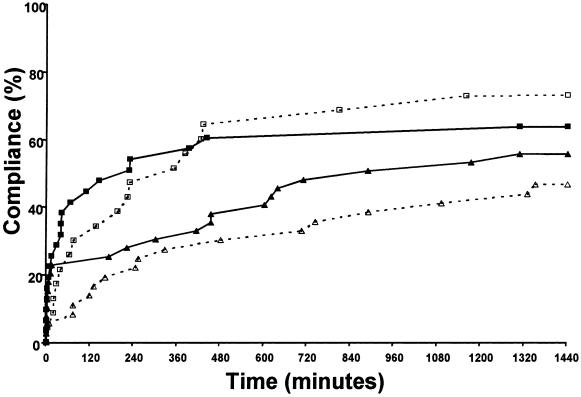
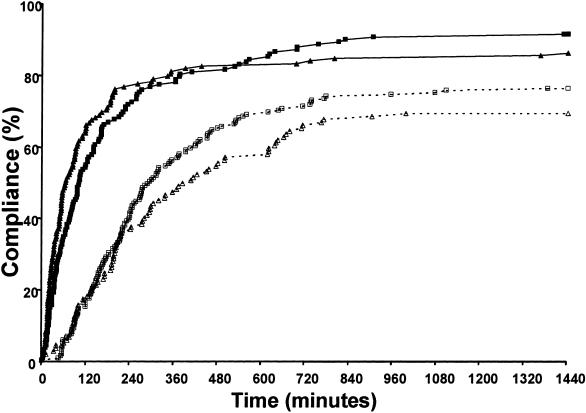
Results: During CPOE, checking for unknown serum values increased after implementation compared with control at one hour: 19% vs. 6% for digoxin, 57% vs. 9% for potassium, and 40% vs. 12% for magnesium as well as at 24 hours (p < 0.01 for all comparisons). Electrolyte supplementation increased with newly reported hypokalemia and hypomagnesemia after implementation at one hour: 35% vs. 6% and 49% vs. 5% for potassium and magnesium, respectively, as well as at 24 hours (p < 0.01 for all comparisons). During CPOE, supplementation for hypokalemia was not improved, whereas supplementation for hypomagnesemia improved at one hour (p < 0.05).
Conclusion: Overall, the alerts improved the safe use of digoxin. During CPOE, alerts associated with missing levels were effective. For hypokalemia and hypomagnesemia, the alerts given during CPOE were not as effective as those given at the time of newly reported low electrolytes.
Figures
References
-
- Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. JAMA. 1997;277:307–11. - PubMed
-
- Classen DC, Pestotnik SL, Evans S, et al. Adverse drug events in hospitalized patients. JAMA. 1997;277:301–6. - PubMed
-
- Johnson JA, Bootman JL. Drug-related morbidity and mortality: a cost-of-illness model. Arch Intern Med. 1995;155:1949–56. - PubMed
-
- Bates DW, Boyle DL, Vander Vliet MD, et al. Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995;10:199–205. - PubMed
-
- Bates DW, Cullen D, Laird N, et al. Incidence of adverse drug events and potential adverse drug events: implications for prevention. JAMA. 1995;274:29–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
