

Risk of complications of pregnancy in women with type 1 diabetes: nationwide prospective study in the Netherlands
- PMID: 15066886
- PMCID: PMC390158
- DOI: 10.1136/bmj.38043.583160.EE
Risk of complications of pregnancy in women with type 1 diabetes: nationwide prospective study in the Netherlands
Abstract
Objective: To investigate maternal, perinatal, and neonatal outcomes of pregnancies in women with type 1 diabetes in the Netherlands.
Design: Nationwide prospective cohort study.
Setting: All 118 hospitals in the Netherlands.
Participants: 323 women with type 1 diabetes who became pregnant between 1 April 1999 and 1 April 2000.
Main outcome measures: Maternal, perinatal, and neonatal outcomes of pregnancy.
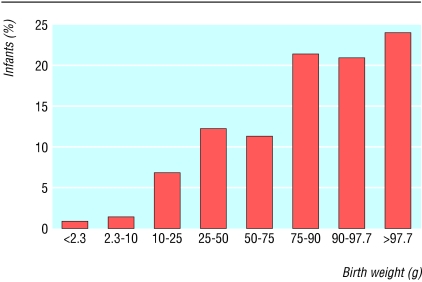
Results: 84% (n = 271) of the pregnancies were planned. Glycaemic control early in pregnancy was good in most women (HbA(1c) < or = 7.0% in 75% (n = 212) of the population), and folic acid supplementation was adequate in 70% (n = 226). 314 pregnancies that went beyond 24 weeks' gestation resulted in 324 infants. The rates of pre-eclampsia (40; 12.7%), preterm delivery (101; 32.2%), caesarean section (139; 44.3%), maternal mortality (2; 0.6%), congenital malformations (29; 8.8%), perinatal mortality (9; 2.8%), and macrosomia (146; 45.1%) were considerably higher than in the general population. Neonatal morbidity (one or more complications) was extremely high (260; 80.2%). The incidence of major congenital malformations was significantly lower in planned pregnancies than in unplanned pregnancies (4.2% (n = 11) v 12.2% (n = 6); relative risk 0.34, 95% confidence interval 0.13 to 0.88).
Conclusion: Despite a high frequency of planned pregnancies, resulting in overall good glycaemic control (early) in pregnancy and a high rate of adequate use of folic acid, maternal and perinatal complications were still increased in women with type 1 diabetes. Neonatal morbidity, especially hypoglycaemia, was also extremely high. Near optimal maternal glycaemic control (HbA1c < or = 7.0%) apparently is not good enough.
Figures
References
-
- Willhoite MB, Bennert HW Jr, Palomaki GE, Zaremba MM, Herman WH, Williams JR, et al. The impact of preconception counseling on pregnancy outcomes: the experience of the Maine diabetes in pregnancy program. Diabetes Care 1993;16: 450-5. - PubMed
-
- Diabetes care and research in Europe: the Saint Vincent declaration. Diabet Med 1990;7: 360. - PubMed
-
- Fuhrmann K, Reiher H, Semmler K, Fischer F, Fischer M, Glockner E. Prevention of congenital malformations in infants of insulin-dependent mothers. Diabetes Care 1983;6: 219-223. - PubMed
-
- Kitzmiller JL, Gavin LA, Gin GD, Jovanovic-Peterson L, Main EK, Zigrang WD. Preconception care of diabetes: glycemic control prevents congenital anomalies. JAMA 1991;265: 731-6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous