

Left regional cardiac perfusion in vitro with platelet-activating factor, norepinephrine and K+ reveals that ischaemic arrhythmias are caused by independent effects of endogenous "mediators" facilitated by interactions, and moderated by paradoxical antagonism
- PMID: 15066909
- PMCID: PMC1574949
- DOI: 10.1038/sj.bjp.0705767
Left regional cardiac perfusion in vitro with platelet-activating factor, norepinephrine and K+ reveals that ischaemic arrhythmias are caused by independent effects of endogenous "mediators" facilitated by interactions, and moderated by paradoxical antagonism
Abstract
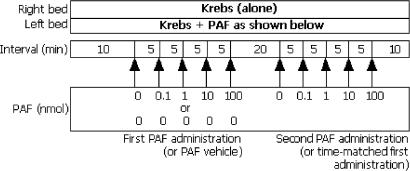
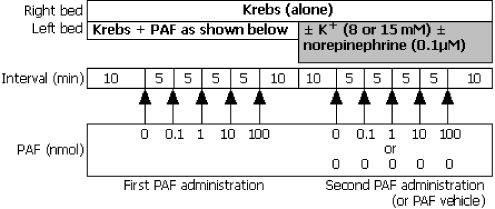
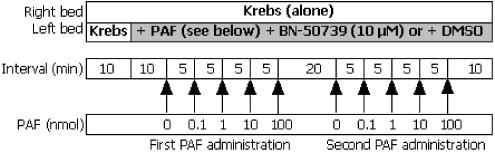
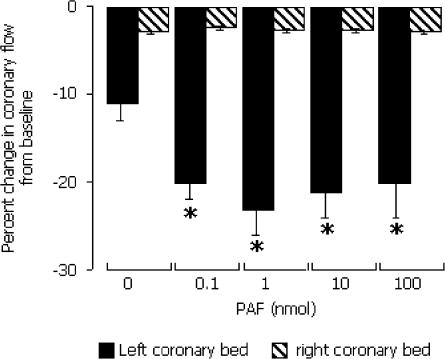
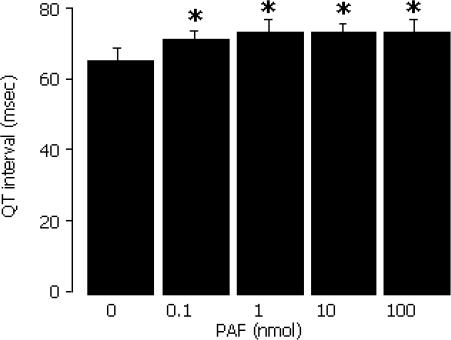
Various putative drug targets for suppression of ischaemia-induced ventricular fibrillation (VF) have been proposed, but therapeutic success in the suppression of sudden cardiac death (SCD) has been disappointing. Platelet-activating factor (PAF) is a known component of the ischaemic milieu. We examined its arrhythmogenic activity, and its interaction with two other putative mediators, norepinephrine and K(+), using an ischaemia-free in vitro heart bioassay, and a specific PAF antagonist (BN-50739). PAF (0.1-100 nmol) was administered selectively to the left coronary bed of rat isolated hearts using a specially designed catheter. In some hearts, PAF was administered to the left coronary bed during concomitant regional perfusion with norepinephrine and/or K(+). In separate studies, PAF accumulation in the perfused cardiac tissue was evaluated using (3)H-PAF. PAF evoked ventricular arrhythmias concentration-dependently (P<0.05). It also widened QT interval and reduced coronary flow selectively in the PAF-exposed left coronary bed (both P<0.05). Two exposures of hearts to PAF were necessary to evoke the QT and rhythm effects. The PAF-induced arrhythmias and coronary vasoconstriction were partially suppressed by the PAF antagonist BN-50739 (10 microm), although BN-50739 itself widened QT interval. K(+) (8 and 15 mm) unexpectedly antagonised the arrhythmogenic effects of PAF without itself eliciting arrhythmias (P<0.05). Norepinephrine (0.1 microm) had little or no effect on the actions of PAF, while failing to evoke arrhythmias itself. Nevertheless, the combination of 15 mm K(+) and 0.1 microm norepinephrine evoked arrhythmias of a severity similar to arrhythmias evoked by PAF alone, without adding to or diminishing the arrhythmogenic effects of PAF. (3)H-PAF accumulated in the cardiac tissue, with 43+/-5% still present 5 min after bolus administration, accounting for the need for two exposures of the heart to PAF for evocation of arrhythmias. Thus, PAF, by activating specific receptors in the ventricle, can be expected to contribute to arrhythmogenesis during ischaemia. However, its interaction with other components of the ischaemic milieu is complex, and selective block of its actions (or its accumulation) in the ischaemic milieu is alone unlikely to reduce VF/SCD.
Figures
References
-
- ALAM I., SMITH J.B., SLIVER M.J. Human and rabbit platelets form platelet activating factor in response to calcium ionophore. Thrombosis Res. 1983;30:71–79. - PubMed
-
- ALLAN G., LEVI R. Thromboxane and prostacyclin release during cardiac immediate hypersensitivity reactions in vitro. J. Pharmacol. Exp. Therap. 1981;217:157–161. - PubMed
-
- ARRIBAS S., MARIN J., PONTE A., BALFAGON G., SALAICES M. Norepinephrine-induced relaxations in rat aorta mediated by endothelial beta-adrenoceptors – impairment by aging and hypertension. J. Pharmacol. Exp. Therap. 1994;270:520–527. - PubMed
-
- AVKIRAN M., CURTIS M.J. Independent dual perfusion of left and right coronary arteries in isolated rat hearts. Am. J. Physiol. 1991;261:H2082–H2090. - PubMed
-
- BAKER K.E., CURTIS M.J. Protection against ventricular fibrillation by the PAF antagonist, BN-50739, involves an ischaemia-selective mechanism. J. Cardiovasc. Pharmacol. 1999;34:394–401. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
