

Three day versus five day treatment with amoxicillin for non-severe pneumonia in young children: a multicentre randomised controlled trial
- PMID: 15070633
- PMCID: PMC383371
- DOI: 10.1136/bmj.38049.490255.DE
Three day versus five day treatment with amoxicillin for non-severe pneumonia in young children: a multicentre randomised controlled trial
Erratum in
- BMJ. 2004 May 1;328(7447):1066
Abstract
Objective: To assess the efficacy of three days versus five days of treatment with oral amoxicillin for curing non-severe pneumonia in children.
Design: Randomised, double blind, placebo controlled multicentre trial.
Setting: Outpatient departments of seven referral hospitals in India.
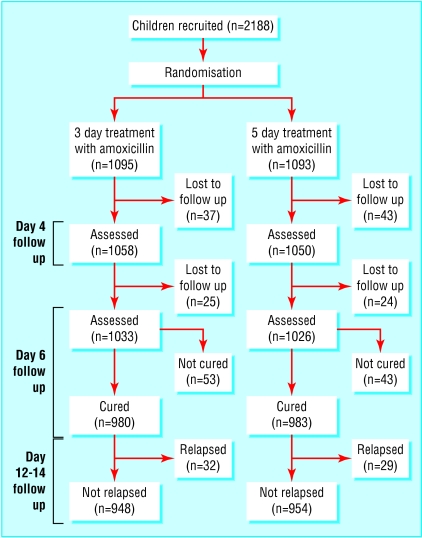
Participants: 2188 children aged 2-59 months, 1095 given three days of treatment and 1093 given five days.
Intervention: Oral amoxicillin 31-54 mg/kg/day in three divided doses.
Main outcome measures: Treatment failure: defined as development of chest indrawing, convulsions, drowsiness, or inability to drink at any time; respiratory rate above age specific cut points on day 3 or later; or oxygen saturation by pulse oximetry < 90% on day 3.
Results: The clinical cure rates with three days and five days of treatment were 89.5% and 89.9%, respectively (absolute difference 0.4 (95% confidence interval--2.1 to 3.0)). Adherence to treatment regimen was 94% and 85% for three day and five day treatments, respectively. Loss to follow up was 5.4% by day 5. There were no deaths, 41 hospitalisations, and 36 minor adverse reactions. There were 225 (10.3%) clinical failures and 106 (5.3%) relapses, and rates were similar in both treatments. At enrollment, 513 (23.4%) children tested positive for respiratory syncytial virus, and Streptococcus pneumoniae and Haemophilus influenzae were isolated from the nasopharynx in 878 (40.4%) and 496 (22.8%) children, respectively. Clinical failure was associated with isolation of respiratory syncytial virus (adjusted odds ratio 1.95 (95% confidence interval 1.0 to 3.8)), excess respiratory rate of > 10 breaths/minute (2.89 (1.83 to 4.55)), and non-adherence with treatment at day 5 (11.57 (7.4 to 18.0)).
Conclusions: Treatment with oral amoxicillin for three days was as effective as for five days in children with non-severe pneumonia.
Figures
Comment in
-
Amoxicillin for non-severe pneumonia in young children: stop skimping, start investing in antibiotic treatment.BMJ. 2004 Jun 26;328(7455):1566-7; author reply 1567. doi: 10.1136/bmj.328.7455.1566-b. BMJ. 2004. PMID: 15217887 Free PMC article. No abstract available.
-
Amoxicillin for non-severe pneumonia in young children: admission to hospital may indicate adverse effects.BMJ. 2004 Jun 26;328(7455):1567; author reply 1567. doi: 10.1136/bmj.328.7455.1567. BMJ. 2004. PMID: 15217890 Free PMC article. No abstract available.
References
-
- Mathers CD, Murray CJL, Lopez AD, Stein C. The global burden of disease 2000 project: objectives, methods, data sources and preliminary results. Evidence and information for policy (EIP). Geneva: World Health Organization, 2001.
-
- World Health Organization. World health report 1999: making a difference. Geneva: WHO, 1999.
-
- Sazawal S, Black ER. Pneumonia case management trials group. Effect of pneumonia case management on mortality in neonates, infants and preschool children. A meta-analysis of community based trials. Lancet Infect Dis 2003;3: 547-56. - PubMed
-
- Invasive Bacterial infection Surveillance (IBIS) Group, INCLEN. Prospective multicentric hospital surveillance of Streptococcus pneumoniae disease in India. Lancet 1999;353: 1216-21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical