

Patterns and distribution of tobacco consumption in India: cross sectional multilevel evidence from the 1998-9 national family health survey
- PMID: 15070637
- PMCID: PMC383376
- DOI: 10.1136/bmj.328.7443.801
Patterns and distribution of tobacco consumption in India: cross sectional multilevel evidence from the 1998-9 national family health survey
Abstract
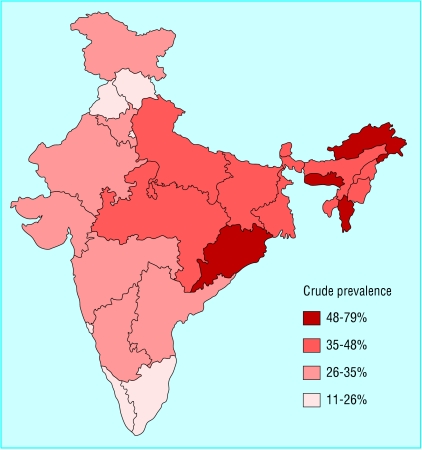
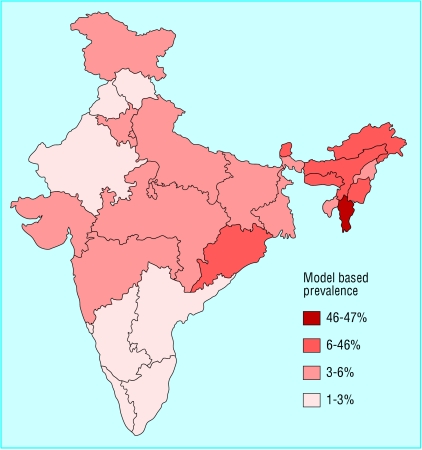
Objective: To investigate the demographic, socioeconomic, and geographical distribution of tobacco consumption in India.
Design: Multilevel cross sectional analysis of the 1998-9 Indian national family health survey of 301 984 individuals in 92 447 households in 3215 villages in 440 districts in 26 states.
Setting: Indian states.
Participants: 301 984 adults (> or = 18 years).
Main outcome measures: Dichotomous variable for smoking and chewing tobacco for each respondent (1 if yes, 0 if no) as well as a combined measure of whether an individual smokes, chews tobacco, or both.
Results: Smoking and chewing tobacco are systematically associated with socioeconomic markers at the individual and household level. Individuals with no education are 2.69 times more likely to smoke and chew tobacco than those with postgraduate education. Households belonging to the lowest fifth of a standard of living index were 2.54 times more likely to consume tobacco than those in the highest fifth. Scheduled tribes (odds ratio 1.23, 95% confidence interval 1.18 to 1.29) and scheduled castes (1.19, 1.16 to 1.23) were more likely to consume tobacco than other caste groups. The socioeconomic differences are more marked for smoking than for chewing tobacco. Socioeconomic markers and demographic characteristics of individuals and households do not account fully for the differences at the level of state, district, and village in smoking and chewing tobacco, with state accounting for the bulk of the variation in tobacco consumption.
Conclusion: The distribution of tobacco consumption is likely to maintain, and perhaps increase, the current considerable socioeconomic differentials in health in India. Interventions aimed at influencing change in tobacco consumption should consider the socioeconomic and geographical determinants of people's susceptibility to consume tobacco.
Figures
Comment in
-
Patterns and distribution of tobacco consumption in India: study should be interpreted cautiously.BMJ. 2004 Jun 19;328(7454):1498; author reply 1499. doi: 10.1136/bmj.328.7454.1498-a. BMJ. 2004. PMID: 15205302 Free PMC article. No abstract available.
-
Patterns and distribution of tobacco consumption in India: impact of religion was not considered.BMJ. 2004 Jun 19;328(7454):1498-9; author reply 1499. doi: 10.1136/bmj.328.7454.1498-b. BMJ. 2004. PMID: 15205303 Free PMC article. No abstract available.
References
-
- World Health Organization. Tobacco or health: a global status report. Geneva: WHO, 1997.
-
- Kumar S. India steps up anti-tobacco measures. Lancet 2000;356: 1089. - PubMed
-
- International Agency for Research on Cancer. Tobacco smoking: monographs on the evaluation of carcinogenic risk of chemicals to humans. Lyons: IARC, 1985.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical