

Gunshot and explosion injuries: characteristics, outcomes, and implications for care of terror-related injuries in Israel
- PMID: 15075646
- PMCID: PMC1356227
- DOI: 10.1097/01.sla.0000114012.84732.be
Gunshot and explosion injuries: characteristics, outcomes, and implications for care of terror-related injuries in Israel
Abstract
Context: An increase of terror-related activities may necessitate treatment of mass casualty incidents, requiring a broadening of existing skills and knowledge of various injury mechanisms.
Objective: To characterize and compare injuries from gunshot and explosion caused by terrorist acts.
Methods: A retrospective cohort study of patients recorded in the Israeli National Trauma Registry (ITR), all due to terror-related injuries, between October 1, 2000, to June 30, 2002. The ITR records all casualty admissions to hospitals, in-hospital deaths, and transfers at 9 of the 23 trauma centers in Israel. All 6 level I trauma centers and 3 of the largest regional trauma centers in the country are included. The registry includes the majority of severe terror-related injuries. Injury diagnoses, severity scores, hospital resource utilization parameters, length of stay (LOS), survival, and disposition.
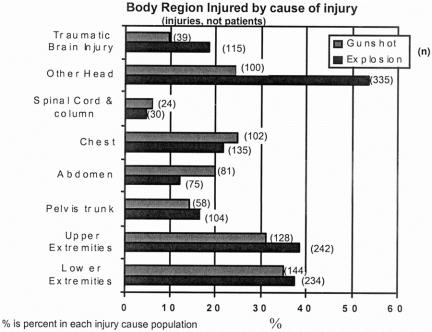
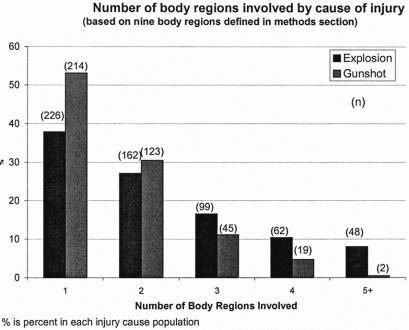
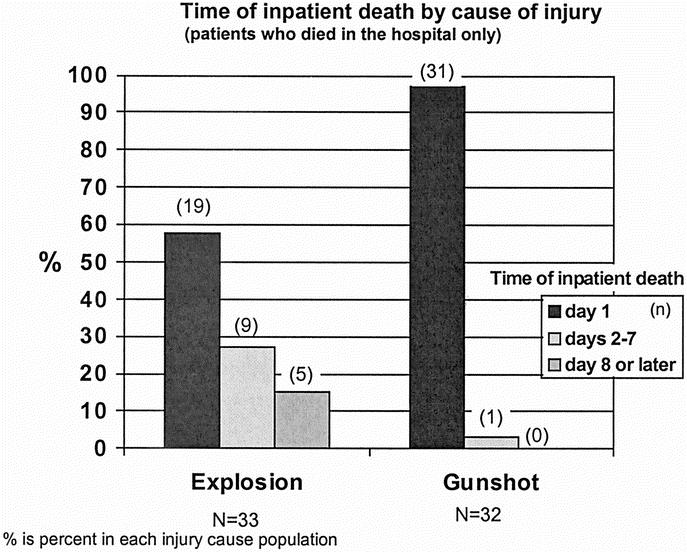
Results: A total of 1155 terror-related injuries: 54% by explosion, 36% gunshot wounds (GSW), and 10% by other means. This paper focused on the 2 larger patient subsets: 1033 patients injured by terror-related explosion or GSW. Seventy-one percent of the patients were male, 84% in the GSW group and 63% in the explosion group. More than half (53%) of the patients were 15 to 29 years old, 59% in the GSW group and 48% in the explosion group. GSW patients suffered higher proportions of open wounds (63% versus 53%) and fractures (42% versus 31%). Multiple body-regions injured in a single patient occurred in 62% of explosion victims versus 47% in GSW patients. GSW patients had double the proportion of moderate injuries than explosion victims. Explosion victims have a larger proportion of minor injuries on one hand and critical to fatal injuries on the other. LOS was longer than 2 weeks for 20% (22% in explosion, 18% in GSW). Fifty-one percent of the patients underwent a surgical procedure, 58% in the GSW group and 46% in explosion group. Inpatient death rate was 6.3% (65 patients), 7.8% in the GSW group compared with 5.3% in the explosion group. A larger proportion of gunshot victims died during the first day (97% versus 58%).
Conclusions: GSW and injuries from explosions differ in the body region of injury, distribution of severity, LOS, intensive care unit (ICU) stay, and time of inpatient death. These findings have implications for treatment and for preparedness of hospital resources to treat patients after a terrorist attack in any region of the world. Tailored protocol for patient evaluation and initial treatment should differ between GSW and explosion victims. Hospital organization toward treating and admitting these patients should take into account the different arrival and injury patterns.
Figures
Comment in
-
Principles of mass casualty management following terrorist disasters.Ann Surg. 2004 Mar;239(3):319-21. doi: 10.1097/01.sla.0000116001.97770.ce. Ann Surg. 2004. PMID: 15075647 Free PMC article. No abstract available.
-
Multiple casualty incidents: lessons from the front line.Ann Surg. 2004 Mar;239(3):322-4. doi: 10.1097/01.sla.0000114220.27301.8f. Ann Surg. 2004. PMID: 15075648 Free PMC article. No abstract available.
References
-
- Stein M, Hirshberg A. Limited mass casualties due to conventional weapons: a daily reality of a level 1 trauma center. In: Terror and Medicine, Shemer J, Shoenfeld Y, eds. Berlin: Pabst Science Publishers, 2003;385.
-
- Frykberg ER, Tepas JJ III, Alexander RH. The 1983 Beirut Airport terrorist bombing. Injury patterns and implications for disaster management. Am Surg. 1989 Mar;55:134–141. - PubMed
-
- Mallonee S, Shariat S, Stennies G, et al. Physical injuries and fatalities resulting from the Oklahoma City bombing. JAMA. 1996;276:382–387. - PubMed
-
- Hanoch J, Feigin E, Pikarsky A, et al. Stab wounds associated with terrorist activities in Israel. JAMA. 1996;276:388–390. - PubMed
-
- Peleg K, Aharonson-Daniel L, Stein M, et al. Patterns of injury in hospitalized terrorist victims. Am J Emerg Med 2003;21:258–262. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
