

Lymphatic mapping and sentinel node biopsy using 99mTc tin colloid in gastric cancer
- PMID: 15075656
- PMCID: PMC1356237
- DOI: 10.1097/01.sla.0000114227.70480.14
Lymphatic mapping and sentinel node biopsy using 99mTc tin colloid in gastric cancer
Abstract
Objective: The aim of this study was to determine the feasibility of sentinel lymph node (SLN) biopsy in patients with gastric cancer for the assessment of regional lymph node status.
Summary background data: SLN is the first draining node from the primary lesion, and it is the first site of lymph node metastasis in malignancy. SLN mapping and biopsy are of great significance in the determination of the extent of lymphadenectomy, allowing patients with gastric cancer to have a better quality of life without jeopardizing survival.
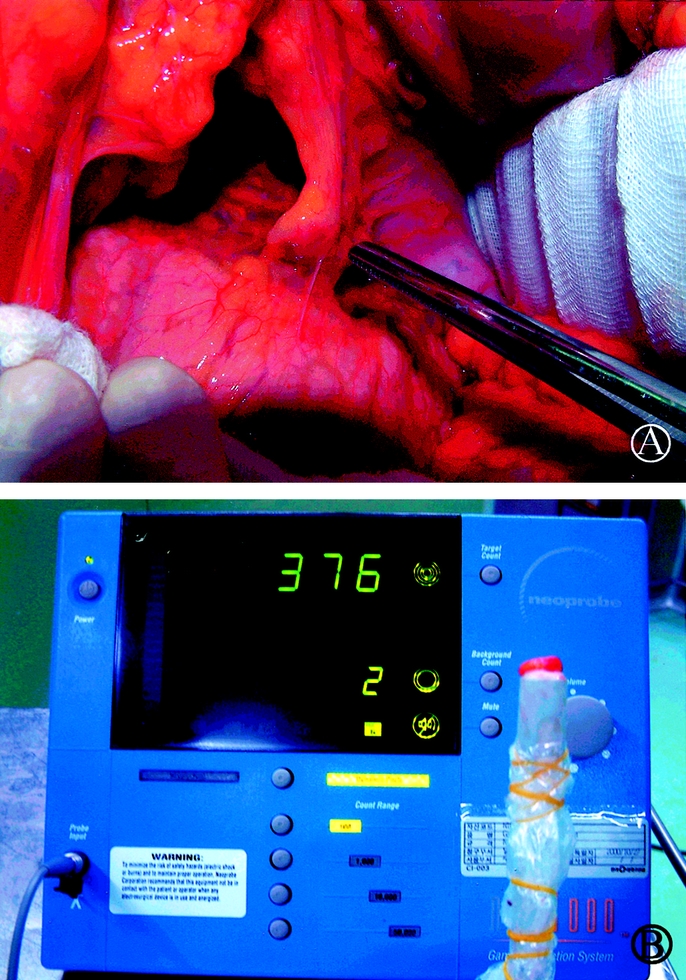
Methods: The SLN biopsy was performed in 46 consecutive patients having gastric cancer with a preoperative imaging stage of T1/T2, N0, or M0. Three hours prior to each operation, Tc tin colloid (2.0 mL, 1.0 mCi) was endoscopically injected into the gastric submucosa around the primary tumor. Subsequently, serial lymphoscintigraphy was performed using a dual-head gamma camera. After the SLN biopsy had been performed using a gamma probe, all patients underwent radical gastrectomy (D2 or D2+alpha). The SLN was cut and immediately frozen-sectioned. A paraffin block was then produced for permanent hematoxylin-eosin staining and immunohistochemistry (IHC).
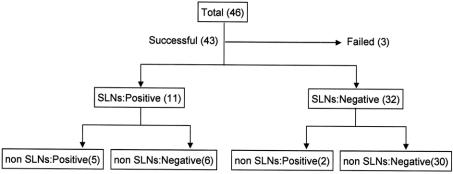
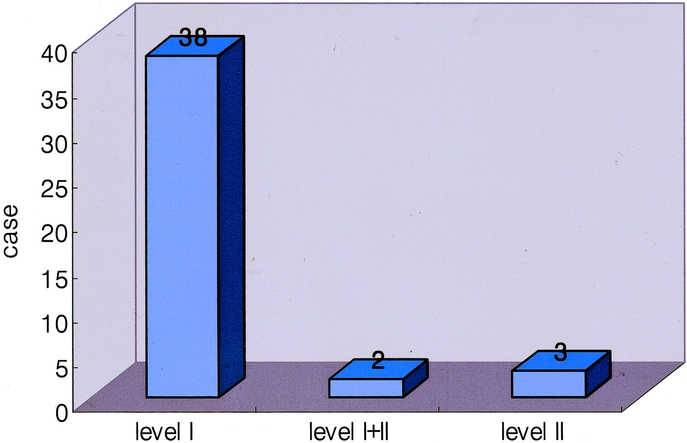
Results: SLNs were successfully identified in 43 of 46 patients (success rate, 93.5%). On average, 2 (range, 1-8) SLNs were identified per patient. The positive predictive value, negative predictive value, sensitivity, and specificity of SLN biopsy were 100% (11 of 11), 93.8% (30 of 32), 84.6% (11 of 13), and 100% (30 of 30), respectively. SLNs were located at the level I lymph nodes in 38 (88.4%), the level I+II nodes in 2 (4.7%), and the level II nodes in 3 (7.0%). No micrometastases of SLNs was found on IHC for cytokeratin.
Conclusions: SLN biopsy using a radioisotope in patients with gastric cancer is a technically feasible and accurate technique, and it is a minimally invasive approach in the assessment of patient nodal status.
Figures
References
-
- Hundley JC, Shen P, Shiver SA, et al. Lymphatic mapping for gastric adenocarcinoma. Am Surg. 2002;8:931–935. - PubMed
-
- Walter L Jr. Surgical management of gastric cancer. In: Silberman H, Silberman AW, eds. Surgical Oncology: Multidisciplinary Approach to Difficult Problems. New York: Arnold; 2002:525–540.
-
- Ajani J, Brand R, Burak WE, et al. Practice Guidelines in Oncology-v. 1. 2002. Gastric cancer. Available at: http://www.nccn.org/physician-gls/index.html. Accessed Dec. 28, 2002.
-
- Hayes N, Karat D, Scott DJ, et al. Radical lymphadenectomy in the management of early gastric cancer. Br J Surg. 1996;83:1421–1423. - PubMed
-
- Maruyama K, Sasako M, Kinoshita T, et al. Can sentinel node biopsy indicate rational extent of lymphadenectomy in gastric cancer surgery? Fundamental and new information on lymph-node dissection. Langenbecks Arch Surg. 1999;384:149–157. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
