

How to diagnose axial spondyloarthritis early
- PMID: 15082484
- PMCID: PMC1754994
- DOI: 10.1136/ard.2003.011247
How to diagnose axial spondyloarthritis early
Abstract
Background: Chronic low back pain (LBP), the leading symptom of ankylosing spondylitis (AS) and undifferentiated axial spondyloarthritis (SpA), precedes the development of radiographic sacroiliitis, sometimes by many years.
Objective: To assign disease probabilities and to develop an algorithm to help in the early diagnosis of axial SpA.
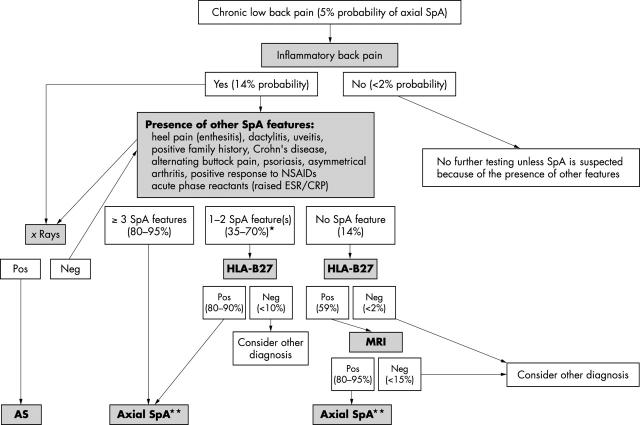
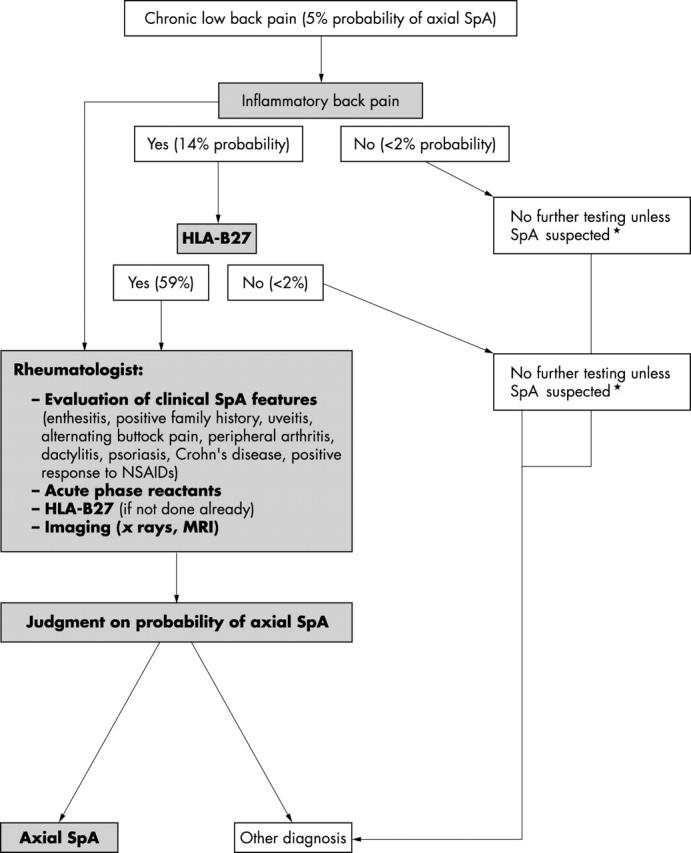
Methods: Axial SpA comprises AS and undifferentiated SpA with predominant axial involvement. Clinical features include inflammatory back pain (IBP), alternating buttock pain, enthesitis, arthritis, dactylitis, acute anterior uveitis, a positive family history, psoriasis, inflammatory bowel disease, and good response to NSAIDs. Associated laboratory findings include raised acute phase reactions, HLA-B27 association, and abnormalities on skeletal imaging. Sensitivities, specificities, and likelihood ratios (LRs) of these parameters were determined from published studies. A 5% prevalence of axial SpA among patients with chronic LBP was used. The probability of the presence of axial SpA, depending on the presence or absence of the above clinical features of SpA, was determined. A probability of > or = 90% was used to make a diagnosis of axial SpA.
Results: The presence of inflammatory back pain features increased the probability of axial SpA from the background 5% prevalence to 14%. The presence of 2-3 SpA features was necessary to increase the probability of axial SpA to 90%. The highest LRs were obtained for HLA-B27 and MRI. Diagnostic algorithms to be used in daily practice were suggested.
Conclusions: This approach can help clinicians to diagnose with a high degree of confidence axial SpA at an early stage in patients with IBP who lack radiographic sacroiliitis.
Figures
Comment in
-
Easy assessment of axial spondyloarthritis (early ankylosing spondylitis) at the bedside.Ann Rheum Dis. 2006 Sep;65(9):1251-2. doi: 10.1136/ard.2005.051045. Ann Rheum Dis. 2006. PMID: 16905586 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
