

In vivo targeting of intestinal and extraintestinal transglutaminase 2 by coeliac autoantibodies
- PMID: 15082580
- PMCID: PMC1774023
- DOI: 10.1136/gut.2003.024836
In vivo targeting of intestinal and extraintestinal transglutaminase 2 by coeliac autoantibodies
Abstract
Background: IgA class serum autoantibodies against type 2 (tissue) transglutaminase (TG2) bind to both intestinal and extraintestinal normal tissue sections in vitro, eliciting endomysial, reticulin, and jejunal antibody reactions. It is not known whether similar binding also occurs in coeliac patients in vivo, and may thereby contribute to disease manifestations.
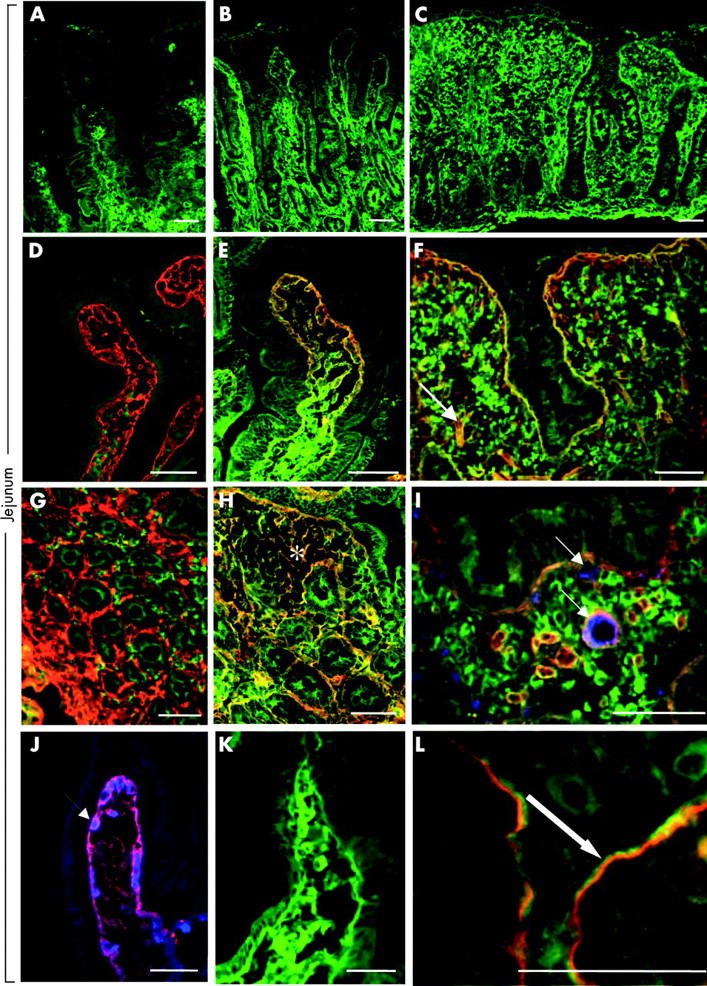
Aims: To investigate intestinal and extraintestinal coeliac tissues for the presence of in vivo bound TG2 specific IgA and its relation to small intestinal mucosal atrophy.
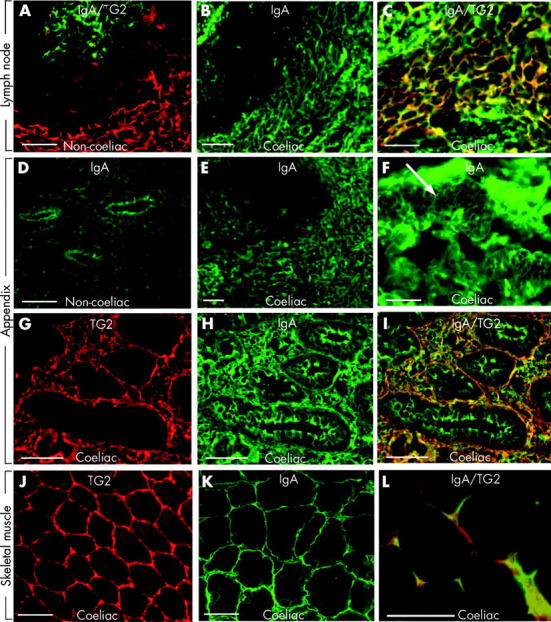
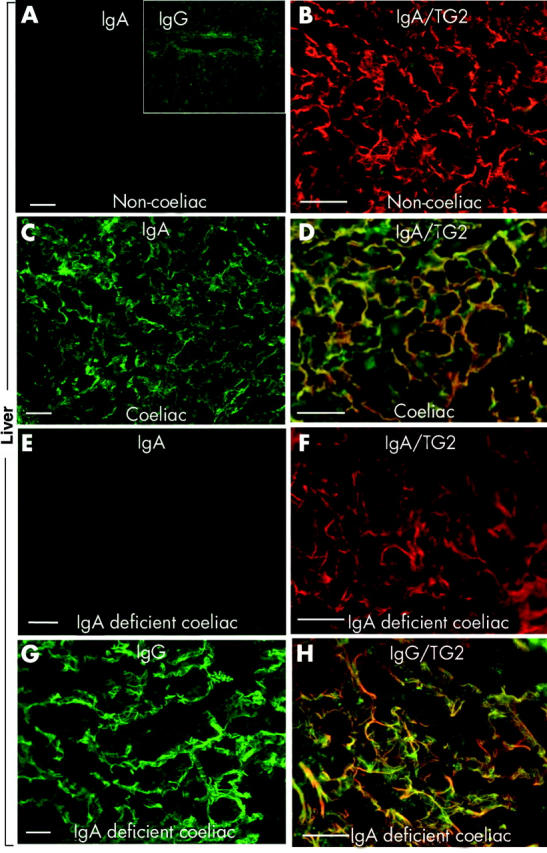
Patients: We investigated jejunal samples with normal villous morphology from 10 patients with developing coeliac disease who subsequently progressed to a flat lesion, from 11 patients with dermatitis herpetiformis, and from 12 non-coeliac controls. Six extrajejunal biopsy samples (liver, lymph node, muscle, appendix), obtained based on independent clinical indications from patients with active coeliac disease, were also studied.
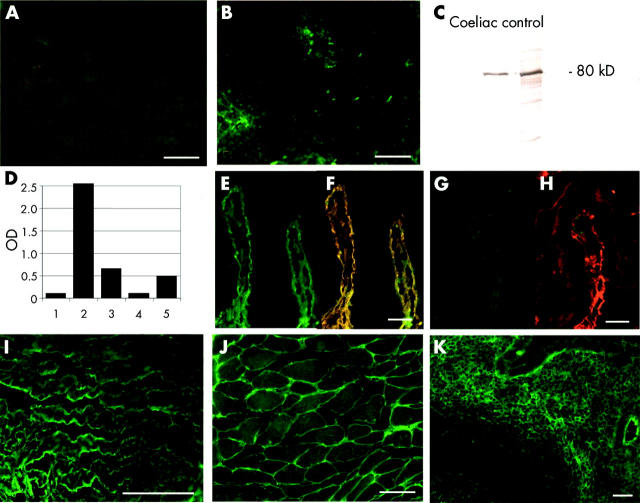
Methods: Double colour immunofluorescent studies for in situ IgA, TG2, and laminin were performed. IgA was eluted from tissue sections and tested for TG2 specificity by enzyme linked immunosorbent assay and indirect immunofluorescence.
Results: IgA (in one IgA deficient case IgG) deposition on extracellularly located TG2 was detected in jejunal and extrajejunal specimens of all coeliac patients, and also in seven of 11 dermatitis herpetiformis patients, of whom two had no circulating endomysial antibodies. IgA eluted from extraintestinal coeliac tissues was targeted against TG2.
Conclusions: Coeliac IgA targets jejunal TG2 early in disease development even when endomysial antibodies are not present in the circulation. Extraintestinal target sites of coeliac IgA further indicate that humoral immunity may have a pathogenetic role.
Figures
References
-
- Mäki M, Collin P. Coeliac disease. Lancet 1997;349:1755–9. - PubMed
-
- Schuppan D. Current concepts of celiac disease pathogenesis. Gastroenterology 2000;119:234–42. - PubMed
-
- Holmes GK. Coeliac disease and malignancy. Dig Liver Dis 2002;34:229–37. - PubMed
-
- Bernstein CN, Leslie WD, Leboff MS. AGA technical review on osteoporosis in gastrointestinal diseases. Gastroenterology 2003;124:795–841. - PubMed
-
- Sher KS, Mayberry JF. Female fertility, obstetric and gynaecological history in coeliac disease: a case control study. Acta Paediatr Suppl 1996;412:76–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous