

Colorectal visceral perception in diverticular disease
- PMID: 15082591
- PMCID: PMC1774033
- DOI: 10.1136/gut.2003.018093
Colorectal visceral perception in diverticular disease
Abstract
Background and aims: The pathogenesis of asymptomatic diverticular disease (ADD) and symptomatic uncomplicated diverticular disease (SUDD) has not been elucidated. The aim of our study was to assess whether altered visceral perception or abnormal compliance of the colorectal wall play a role in these clinical entities.
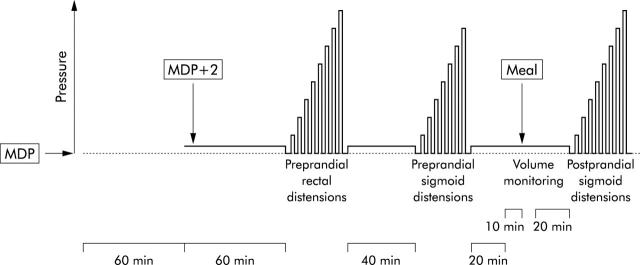
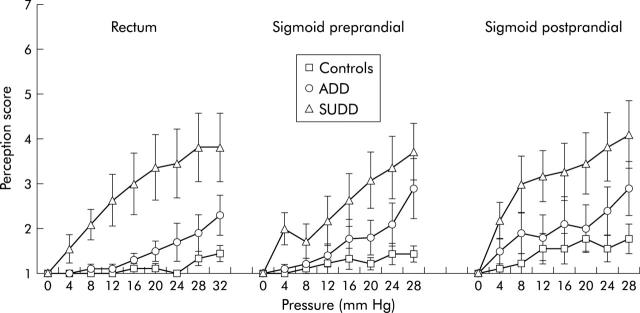
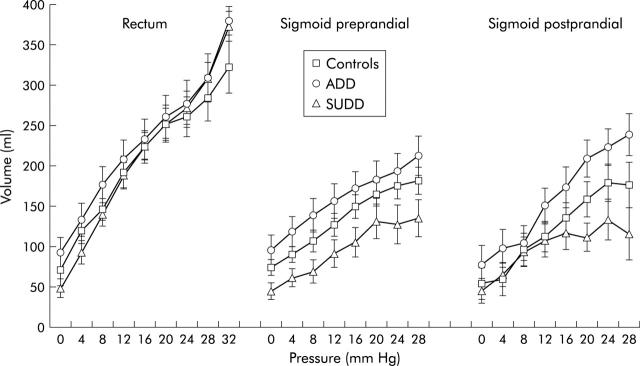
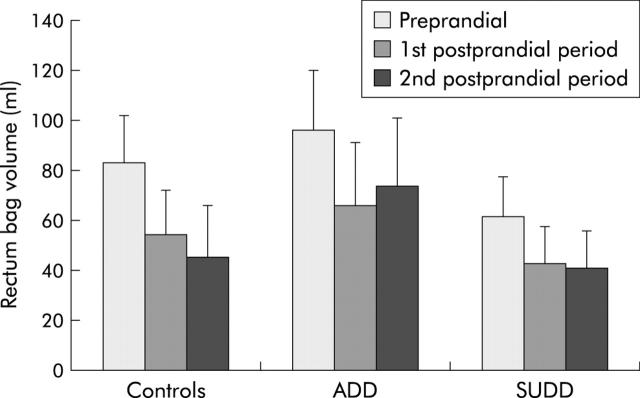
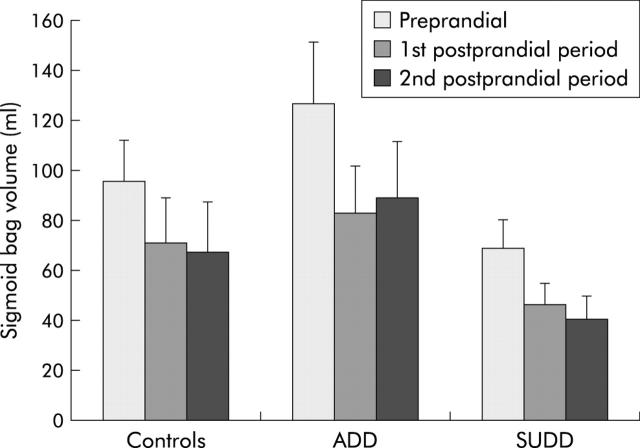
Methods: Ten ADD patients, 11 SUDD patients, and nine healthy controls were studied. Using a dual barostat device, sensations were scored and compliance curves obtained using stepwise intermittent isobaric distensions of the rectum and sigmoid, before and after a liquid meal. In addition, the colonic response to eating was assessed by monitoring the volumes of both barostat bags at operating pressure before and after the meal.
Results: In the rectum, perception was increased in the SUDD group compared with controls (p = 0.010) and the ADD group (p = 0.030). Rectal compliance curves were not different between the groups. In the sigmoid colon, perception in the pre- and postprandial periods was increased in SUDD compared with controls (p = 0.018) but not when compared with ADD. Sigmoid volume-pressure curves had comparable slopes (compliance) in all groups but were shifted downwards in SUDD compared with ADD in the preprandial period (p = 0.026). The colonic response to eating (decrease in intrabag volume) was similar in all three groups, both in the rectum and sigmoid.
Conclusion: Symptomatic but not asymptomatic uncomplicated diverticular disease is associated with heightened perception of distension, not only in the diverticula bearing sigmoid, but also in the unaffected rectum. This hyperperception is not due to altered wall compliance.
Figures
References
-
- Connell AM. Pathogenesis of diverticular disease of the colon. Adv Intern Med 1977;22:377–95. - PubMed
-
- Painter NS, Burkitt DP. Diverticular disease of the colon, a 20th century problem. Clin Gastroenterol 1975;4:2–21. - PubMed
-
- Almy TP, Howell DA. Diverticular disease of the colon. New Engl J Med 1980;302:324–31. - PubMed
-
- Whiteway J, Morson BC. Pathology of the ageing—diverticular disease. Clin Gastroenterol 1985;14:829–46. - PubMed
-
- Cheskin LJ, Lamport RD. Diverticular disease. Epidemiology and pharmacological treatment. Drugs Aging 1995;6:55–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical