

Broad-based general surgery training is a model of continued utility for the future
- PMID: 15082966
- PMCID: PMC1356270
- DOI: 10.1097/01.sla.0000124384.08410.94
Broad-based general surgery training is a model of continued utility for the future
Abstract
Summary background data: Our program has emphasized broad-based training that potentially allows residents to pursue a variety of career paths, with or without additional surgical training. Diverse experiences have emphasized a variety of rotations, including a university hospital with a large trauma service, several tertiary private institutions, and suburban and rural experiences with private practitioners. Our faculty includes surgeons with both broad-based and narrowly focused practices. In light of duty-hour restrictions and proposed changes in surgical training, we assessed the results of this model over an extended period.
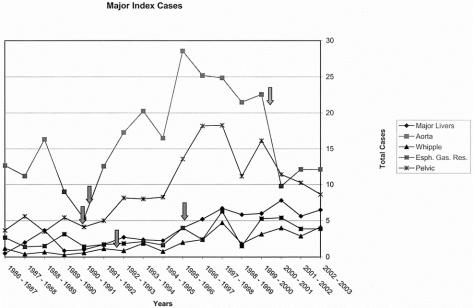
Materials and methods: The case volume from the Residency Review Committee (RRC) operative logs, ABSITE scores, ABS performance, fellowship training, and subsequent career choices were examined for all graduating chief residents in general surgery from our program over the past 17 years. The impact of specialty faculty was assessed and data from 5 index (aortic, major esophagogastric, liver, pancreatic, and pelvic resections) cases were also abstracted from the logs. A survey was then sent to all 208 of the 212 surgeons who had completed the program since 1971.
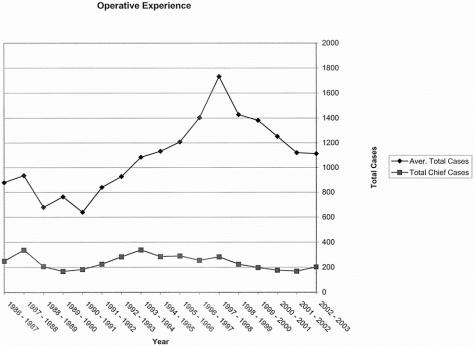
Results: Of the 115 residents who completed training in the last 17 years, 60 pursued fellowship training and 55 went directly into general surgical practice in 20 states. Fifteen of the 29 residents who had an elective laboratory experience were among the 23 who remained in academic careers. The operative experience has been excellent (1090 +/- 42 total major; 240 +/- 21 surgeon chief). Experience did not vary, even though the number of graduating chiefs ranged from 5 to 8 per year, and there have been no deficiencies in RRC index cases. The addition of specialty faculty (n = 5) at various intervals promptly increased the volume of complex cases in pelvic, liver, pancreas, and vascular surgery. Since all residents promptly passed the ABS examinations, it was not possible to discern factors associated with Board performances other than broad-based training. The survey demonstrated that most continued to practice broad-based general surgery and believed that such training was highly relevant to their current practice.
Conclusions: The provision of broad-based training with generalists and specialty faculty has allowed for excellent breadth and depth in case volume. While many residents pursued fellowships, those who did not have indeed achieved successful careers. Most continue to practice general surgery, indicating the value of complete training in this field. It will be important to monitor these outcomes as changes in residency training occur.
Figures
References
-
- Polk HC Jr. Challenges in surgical education, competencies, work hours, and workforce. Assessment and adaption. Am J Surg. 2002;184:225–253. - PubMed
-
- Richardson JD. Workforce and lifestyle issues in general surgery training and practice. Arch Surg. 2002;137:515–520. - PubMed
-
- Knapp R. Financing graduate medical education and limiting resident work hours: a political assessment. Am J Surg. 2002;184:187–195. - PubMed
-
- Bland KI, Isaacs G. Contemporary trends in student selection of medical specialties. Arch Surg. 2002;137:259–267. - PubMed
-
- Itani K. A positive approach to core competencies and benchmarks for graduate medical education. Am J Surg. 2002;184:196–203. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
