

Clinical genetic testing and early surgical intervention in patients with multiple endocrine neoplasia type 1 (MEN 1)
- PMID: 15082967
- PMCID: PMC1356271
- DOI: 10.1097/01.sla.0000124383.98416.8d
Clinical genetic testing and early surgical intervention in patients with multiple endocrine neoplasia type 1 (MEN 1)
Abstract
Objective: We sought to develop a comprehensive program for clinical genetic testing in a large group of extended families with multiple endocrine neoplasia type 1 (MEN 1), with the ultimate aim of early tumor detection and surgical intervention.
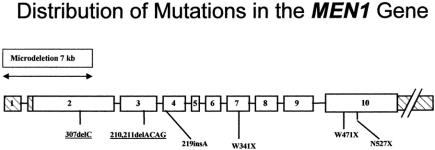
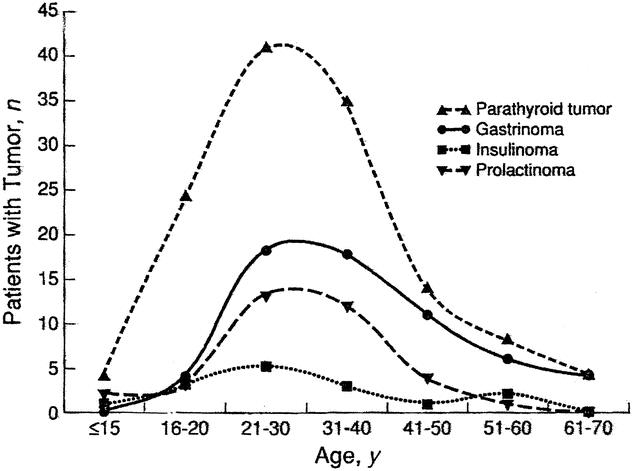
Summary background data: Germline mutations in the MEN1 tumor suppressor gene are responsible for the MEN 1 syndrome. Direct genetic testing for a disease-associated MEN1 mutation is now possible in selected families. The neuroendocrine tumors of the pancreas/duodenum and the intrathoracic neuroendocrine tumors that occur in MEN 1 carry a malignant potential. Importantly, these tumors arise in otherwise young healthy patients and are complicated by the potential for multifocality and involvement of multiple target tissues. The optimal screening methods and indications for early surgical intervention in genetically positive patients have yet to be defined.
Methods: Nine MEN 1 kindreds were included in the study. The mutations for each kindred were initially identified in the research laboratory. Subsequently, mutation detection was independently validated in the clinical Molecular Diagnostic Laboratory. Each patient in the study underwent formal genetic counseling before testing.
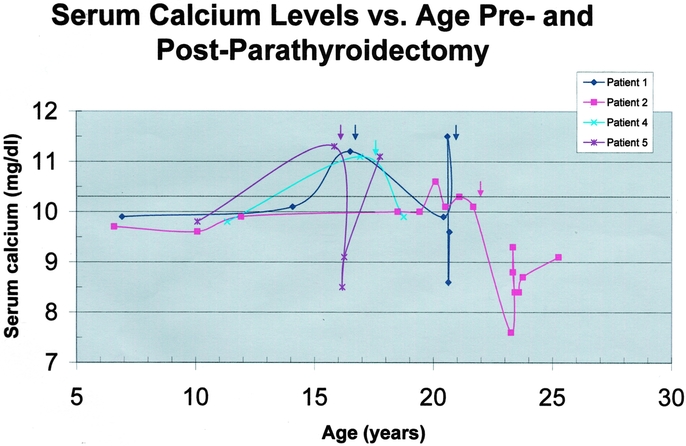
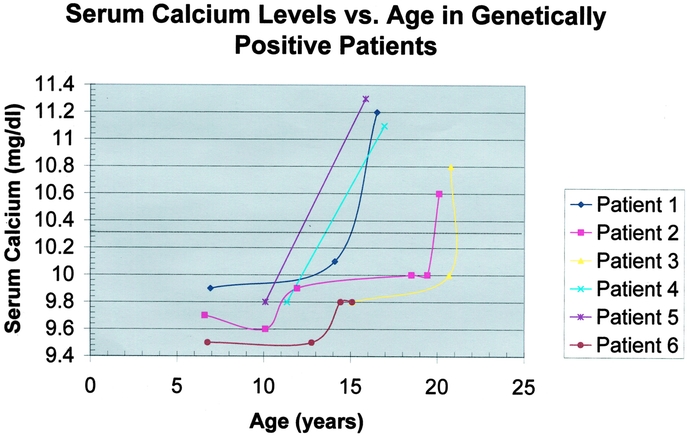
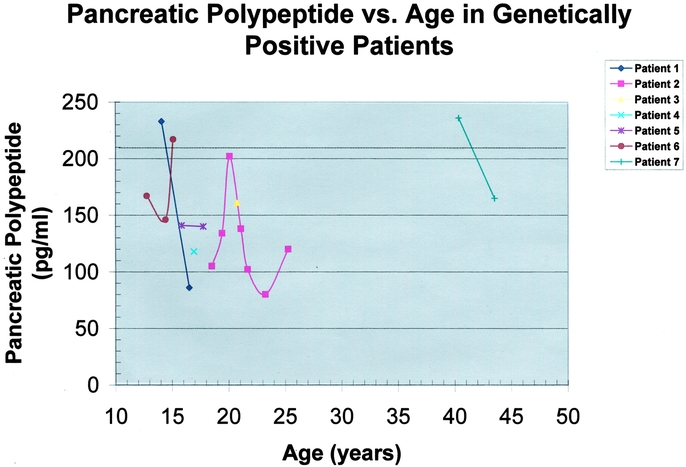
Results: Genetic testing was performed in 56 at-risk patients. Patients were stratified according to risk: Group I (n = 25), 50% risk, younger than 30 years old; Group II (n = 20), 50% risk, 30 years old or older; Group III (n = 11) 25% risk. Seven patients (age, 12 to 42 years; mean, 20.6 +/- 3.8 years) had a positive genetic test. Patients with a novel positive genetic test were in either Group I (n = 6) or Group II (n = 1) and have been followed for 35.8 +/- 2.0 months. Of the 7 genetically positive patients, hypercalcemia was either present at the time of diagnosis or developed during the period of follow-up in 6 patients. Four patients have undergone parathyroidectomy as early as age 16 years. One genetically positive patient has not yet developed hyperparathyroidism. Intensive biochemical screening in this select group of patients identified an elevated pancreatic polypeptide level and pancreatic tail mass lesion in a 15-year-old male who is asymptomatic and currently normocalcemic.
Conclusions: Genetic testing identifies patients harboring an MEN1 mutation before the development of clinical signs or symptoms of endocrine disease. When genetically positive patients are carefully studied prospectively, biochemical evidence of neoplasia can be detected an average of 10 years before clinically evident disease, allowing for early surgical intervention. Genetically positive individuals should undergo focused cancer surveillance for early detection of the potentially malignant neuroendocrine tumors that account for most of the disease-related morbidity and mortality.
Figures
References
-
- Marx S, Spiegel AM, Skarulis MC, et al. Multiple endocrine neoplasia type 1: Clinical and genetic topics. Ann Intern Med. 1998;129:484–494. - PubMed
-
- Ballard HS, Frame B, Hartsock RJ. Familial multiple endocrine adenoma-peptic ulcer complex. Medicine. 1964;43:481–516. - PubMed
-
- Wilkinson S, Teh BT, Davey KR, et al. Cause of death in multiple endocrine neoplasia type 1. Arch Surg. 1993;128:683. - PubMed
-
- Doherty GM, Olson JA, Frisella MM, et al. Lethality of multiple endocrine neoplasia type 1. World J Surg. 1997;22:581–586. - PubMed
-
- Chandrasekharappa SC, Guru SC, Manickamp P, et al. Positional cloning of the gene for multiple endocrine neoplasia-type 1. Science. 1997;276:404–407. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
