

Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection
- PMID: 15082972
- PMCID: PMC1356276
- DOI: 10.1097/01.sla.0000124386.54496.15
Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection
Abstract
Objective: To describe clinical characteristics and outcomes of a large cohort of intraductal papillary mucinous neoplasms (IPMNs) of the pancreas affecting the main pancreatic duct.
Summary background data: IPMNs are being diagnosed with increasing frequency. Preoperative determination of malignancy remains problematic, and reported results of long-term survival following resection are conflicting.
Methods: The combined databases from the Massachusetts General Hospital and the Pancreatic Unit of the University of Verona were analyzed. To avoid confusing overlap with mucinous cystic neoplasms, only patients with tumors of the main pancreatic duct (with or without side branch involvement) were included. A total of 140 tumors consecutively resected between 1990 and 2002 were classified as either benign (adenoma and borderline tumors) or malignant (carcinoma in situ or invasive cancer) to compare their characteristics and survival.
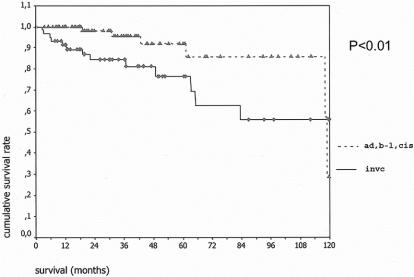
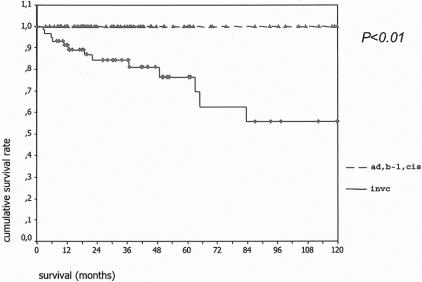
Results: Men and women were equally affected (mean age 65 years). Seven patients (12%) had adenomas, 40 (28%) borderline tumors, 25 (18%) carcinoma in situ, and 58 (42%) invasive carcinoma. The median age of patients with benign IPMN was 6.4 years younger than those with malignant tumors (P = 0.04). The principal symptoms were abdominal pain (65%), weight loss (44%), acute pancreatitis (23%), jaundice (17%), and onset or worsening of diabetes (12%); 27% of patients were asymptomatic. Jaundice and diabetes were significantly associated with malignant tumors. Five- and 10-year cancer-specific survival for patients with noninvasive tumors was 100%, and comparable survival of the 58 patients with invasive carcinoma was 60% and 50%.
Conclusions: Cancer is found in 60% of patients with main-duct IPMNs. Patients with malignant tumors are 6 years older than their benign counterparts and have a higher likelihood of presenting with jaundice or new onset diabetes. No patients with benign tumors or carcinoma in situ died of their disease following resection, and those with invasive cancer had a markedly better survival (60% at 5 years) than pancreatic ductal adenocarcinoma. These findings support both the concept of progression of benign IPMNs to invasive cancer and an aggressive policy of resection at diagnosis.
Figures
Comment in
-
IPMN: not a new kid on the block anymore.Gastroenterology. 2004 Dec;127(6):1853-5. doi: 10.1053/j.gastro.2004.10.035. Gastroenterology. 2004. PMID: 15578527 No abstract available.
References
-
- Adsay NV. The “new kid on the block”: intraductal papillary mucinous neoplasms of the pancreas. Current concepts and controversies. Surgery. 2003;133:459–463. - PubMed
-
- Terris B, Ponsot P, Paye F, et al. Intraductal papillary mucinous tumors of the pancreas confined to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol. 2000;24:1372–1377. - PubMed
-
- Kobari M, Egawa S, Shibuya K, et al. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg. 1999;134:1131–1136. - PubMed
-
- Matsumoto T, Aramaki M, Yada K, et al. Optimal management of the branch duct type intraductal papillary mucinous neoplasms of the pancreas. J Clin Gastroenterol. 2003;36:261–265. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
