

Clinical evidence for cervical myelopathy due to Chiari malformation and spinal stenosis in a non-randomized group of patients with the diagnosis of fibromyalgia
- PMID: 15083352
- PMCID: PMC3476600
- DOI: 10.1007/s00586-004-0672-x
Clinical evidence for cervical myelopathy due to Chiari malformation and spinal stenosis in a non-randomized group of patients with the diagnosis of fibromyalgia
Abstract
Objective: While patients with fibromyalgia report symptoms consistent with cervical myelopathy, a detailed neurological evaluation is not routine. We sought to determine if patients with fibromyalgia manifest objective neurological signs of cervical myelopathy.
Methods: Two hundred and seventy patients, 18 years and older, who carried the diagnosis of fibromyalgia but who had no previously recognized neurological disease underwent detailed clinical neurological and neuroradiological evaluation for the prevalence of objective evidence of cervical myelopathy and radiological evidence of cerebellar tonsillar herniation (Chiari 1 malformation) or cervical spinal canal stenosis.
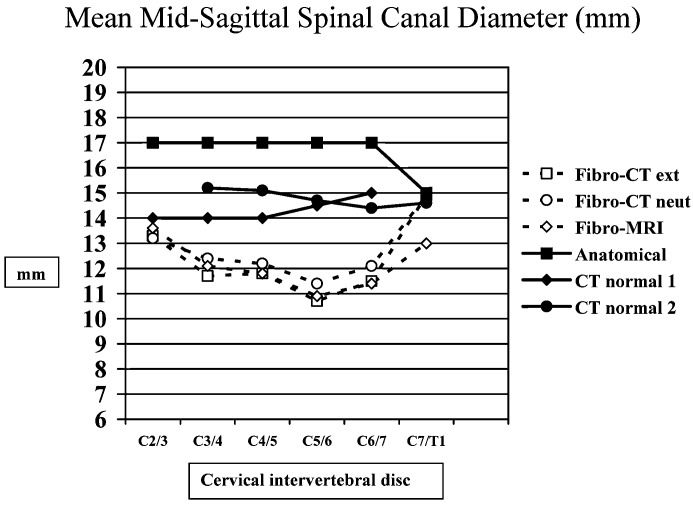
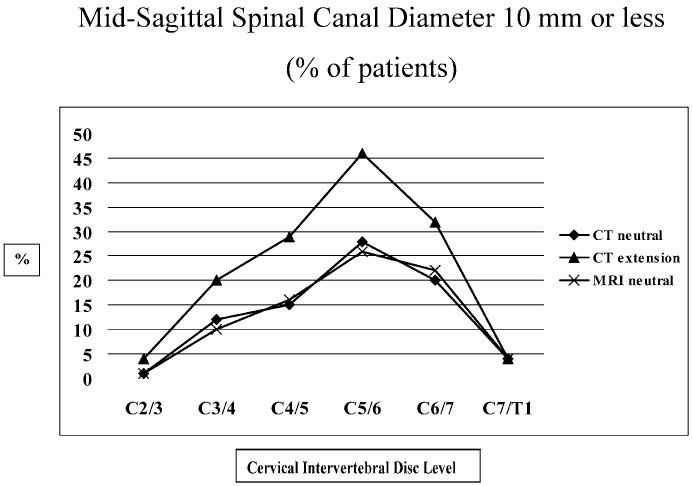
Results: Patients were primarily women (87%), of mean age 44 years, who had been symptomatic for 8 years (standard deviation, 6.3 years). The predominant complaints were neck/back pain (95%), fatigue (95%), exertional fatigue (96%), cognitive impairment (92%), instability of gait (85%), grip weakness (83%), paresthesiae (80%), dizziness (71%) and numbness (69%). Eighty-eight percent of patients reported worsening symptoms with neck extension. The neurological examination was consistent with cervical myelopathy: upper thoracic spinothalamic sensory level (83%), hyperreflexia (64%), inversion of the radial periosteal reflex (57%), positive Romberg sign (28%), ankle clonus (25%), positive Hoffman sign (26%), impaired tandem walk (23%), dysmetria (15%) and dysdiadochokinesia (13%). MRI and contrast-enhanced CT imaging of the cervical spine revealed stenosis. The mean antero-posterior (AP) spinal canal diameter at C2/3, C3/4, C4/5, C5/6, C6/7 and C7/T1 was 13.5 mm, 11.8 mm, 11.5 mm, 10.4 mm, 11.3 mm and 14.5 mm respectively, (CT images). In 46% of patients, the AP spinal diameter at C5/6 measured 10 mm, or less, with the neck positioned in mild extension, i.e., clinically significant spinal canal stenosis. MRI of the brain revealed tonsillar ectopia >5 mm in 20% of patients (mean=7.1+/-1.8 mm), i.e., Chiari 1 malformation. CONCLUSION. Our findings indicate that some patients who carry the diagnosis of fibromyalgia have both signs and symptoms consistent with cervical myelopathy, most likely resulting from spinal cord compression. We recommend detailed neurological evaluation of patients with fibromyalgia in order to exclude cervical myelopathy, a potentially treatable condition.
Figures
References
-
- An HS (1998) Clinical presentation of discogenic neck pain, radiculopthy and myelopathy. In: The Cervical Spine Research Society (editorial committee) The cervical spine, 3rd edn. Lippincott-Raven, Philadelphia, pp 755–764
-
- Arroyo J Rheumatol. 1993;20:1925. - PubMed
-
- Barsky Ann Intern Med. 1999;130:910. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
