

Review
doi: 10.1172/JCI21681.
The emergence of Lyme disease
Affiliations
- PMID: 15085185
- PMCID: PMC385417
- DOI: 10.1172/JCI21681
Item in Clipboard
Review
The emergence of Lyme disease
J Clin Invest.
2004 Apr.
Abstract
Since its identification nearly 30 years ago, Lyme disease has continued to spread, and there have been increasing numbers of cases in the northeastern and north central US. The Lyme disease agent, Borrelia burgdorferi, causes infection by migration through tissues, adhesion to host cells, and evasion of immune clearance. Both innate and adaptive immune responses, especially macrophage- and antibody-mediated killing, are required for optimal control of the infection and spirochetal eradication. Ecological conditions favorable to the disease, and the challenge of prevention, predict that Lyme disease will be a continuing public health concern.
Figures
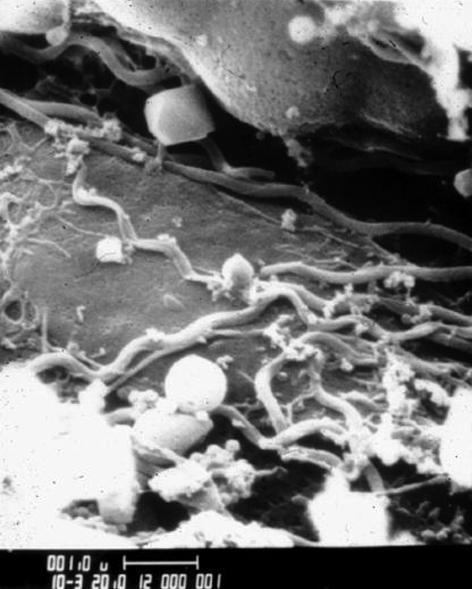
A scanning electron micrograph of B. burgdorferi spirochetes in the midgut of a nymphal I. scapularis tick. The picture is a kind gift of Willy Burgdorfer.
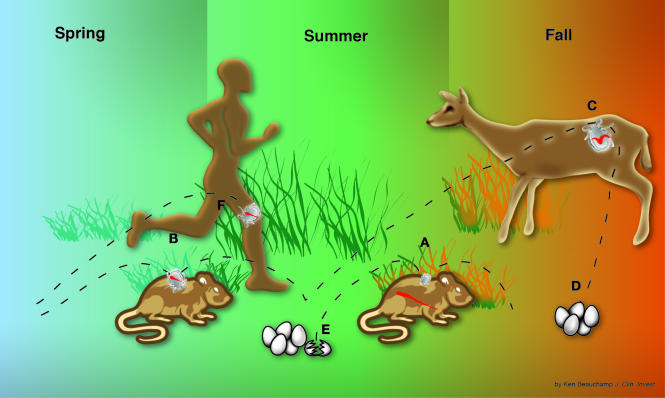
The enzootic cycle of B. burgdorferi infection in the northeastern US and intersection with human Lyme disease. I. scapularis ticks feed once during each of the three stages of their usual 2-year life cycle. Typically, larval ticks take one blood meal in the late summer (A), nymphs feed during the following late spring and early summer (B), and adults feed during the fall (C), after which the female tick lays eggs (D) that hatch the next summer (E). It is critical that the tick feeds on the same host species in both of its immature stages (larval and nymphal), because the life cycle of the spirochete (wavy red line) depends on horizontal transmission: in the early summer, from infected nymphs to certain rodents, particularly mice or chipmunks (B); and in the late summer, from infected rodents to larvae (A), which then molt to become infected nymphs that begin the cycle again in the following year. Therefore, B. burgdorferi spends much of its natural cycle in a dormant state in the midgut of the tick. During the summer months, after transmission to rodents, the spirochete must evade the immune response long enough to be transferred to feeding larval ticks. Although the tick may attach to humans at all three stages, it is primarily the tiny nymphal tick (∼1 mm) that transmits the infection (F). This stage of the tick life cycle has a peak period of questing in the weeks surrounding the summer solstice. Humans are an incidental host and are not involved at all in the life cycle of the spirochete.
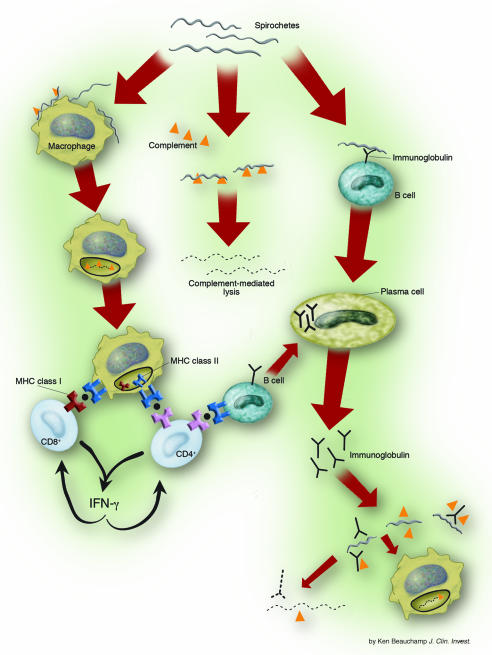
Host mechanisms of spirochetal killing. Complement-mediated lysis of the organism may be the first line of host defense. Spirochetal lipoproteins and other spirochetal signals activate macrophages, leading to the production of strong proinflammatory cytokines, especially TNF-α and IL-1β. Macrophages engulf spirochetes and degrade them in intracellular compartments. Spirochetal lipoproteins, which are B cell mitogens, also stimulate adaptive T cell–independent B cell responses. Humoral immune responses to nonlipidated spirochetal proteins are more likely to be T cell dependent. The primary role of B. burgdorferi–specific CD4+ Th1 cells is to prime T cell–dependent B cell responses, and antigen-specific CD8+ T cells may be a significant source of IFN-γ. Antibody-mediated spirochetal killing occurs by complement fixation and opsonization.
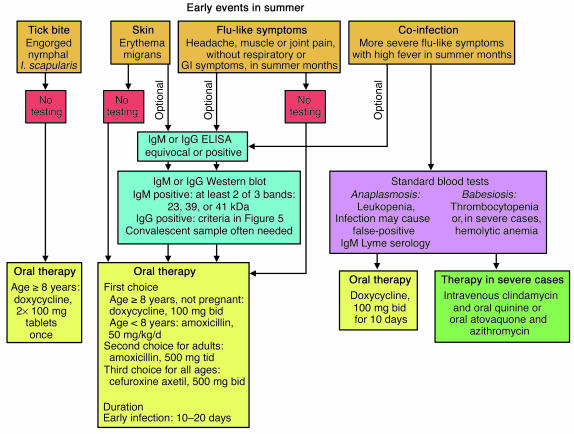
An algorithm for the diagnosis and treatment of the early events surrounding Lyme disease in the summer months. Serologic testing for Lyme disease has limited utility during the first 1 or 2 weeks of infection, and early treatment, without serologic testing, is recommended. If serologic testing is done, acute and convalescent samples should be obtained. GI, gastrointestinal.
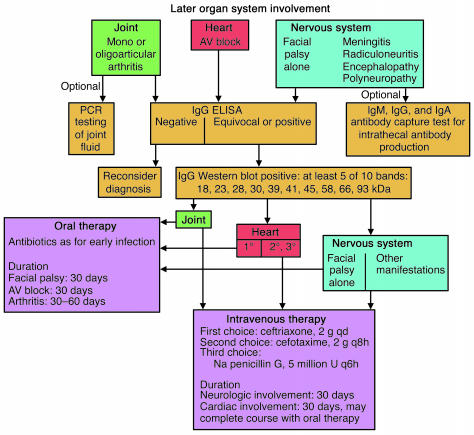
An algorithm for the diagnosis and treatment of late organ-system involvement in Lyme disease. By the time that organ-system involvement is present, which is at least several weeks after the onset of infection, almost all patients have a positive IgG response to B. burgdorferi. Depending on the manifestation, treatment with either oral or intravenous antibiotic therapy is recommended.
References
-
- Steere AC. Lyme disease. N. Engl. J. Med. 2001;345:115–125. - PubMed
-
- Dennis, D.T., and Hayes, E.B. 2002. Epidemiology of Lyme Borreliosis. In Lyme borreliosis: biology, epidemiology and control. O. Kahl, J.S. Gray, R.S. Lane, and G. Stanek, editors. CABI Publishing. Oxford, United Kingdom. 251–280.
-
- Lyme disease: United States, 2000. Morb. Mortal. Wkly. Rep. 2002;51:29–31. - PubMed
-
- Steere AC. Lyme disease. N. Engl. J. Med. 1989;321:586–596. - PubMed
-
- Spielman A. The emergence of Lyme disease and human babesiosis in a changing environment. Ann. N. Y. Acad. Sci. 1994;740:146–156. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
