

Oral rehydration versus intravenous therapy for treating dehydration due to gastroenteritis in children: a meta-analysis of randomised controlled trials
- PMID: 15086953
- PMCID: PMC419333
- DOI: 10.1186/1741-7015-2-11
Oral rehydration versus intravenous therapy for treating dehydration due to gastroenteritis in children: a meta-analysis of randomised controlled trials
Abstract
Background: Despite treatment recommendations from various organizations, oral rehydration therapy (ORT) continues to be underused, particularly by physicians in high-income countries. We conducted a systematic review of randomised controlled trials (RCTs) to compare ORT and intravenous therapy (IVT) for the treatment of dehydration secondary to acute gastroenteritis in children.
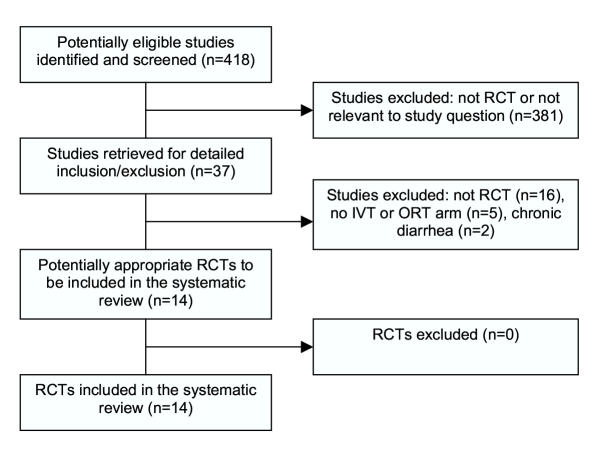
Methods: RCTs were identified through MEDLINE, EMBASE, CENTRAL, authors and references of included trials, pharmaceutical companies, and relevant organizations. Screening and inclusion were performed independently by two reviewers in order to identify randomised or quasi-randomised controlled trials comparing ORT and IVT in children with acute diarrhea and dehydration. Two reviewers independently assessed study quality using the Jadad scale and allocation concealment. Data were extracted by one reviewer and checked by a second. The primary outcome measure was failure of rehydration. We analyzed data using standard meta-analytic techniques.
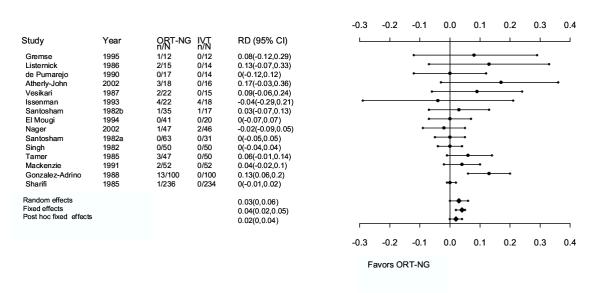
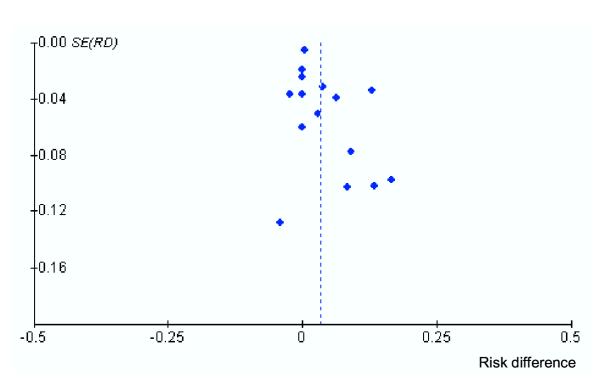
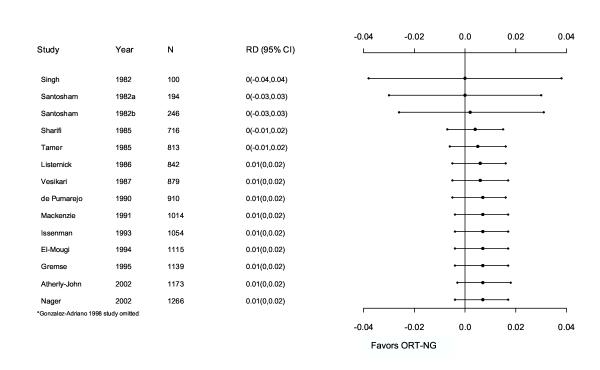
Results: The quality of the 14 included trials ranged from 0 to 3 (Jadad score); allocation concealment was unclear in all but one study. Using a random effects model, there was no significant difference in treatment failures (risk difference [RD] 3%; 95% confidence intervals [CI]: 0, 6). The Mantel-Haenzsel fixed effects model gave a significant difference between treatment groups (RD 4%; 95% CI: 2, 5) favoring IVT. Based on the four studies that reported deaths, there were six in the IVT groups and two in ORT. There were no significant differences in total fluid intake at six and 24 hours, weight gain, duration of diarrhea, or hypo/hypernatremia. Length of stay was significantly shorter for the ORT group (weighted mean difference [WMD] -1.2 days; 95% CI: -2.4,-0.02). Phlebitis occurred significantly more often with IVT (number needed to treat [NNT] 33; 95% CI: 25,100); paralytic ileus occurred more often with ORT (NNT 33; 95% CI: 20,100). These results may not be generalizable to children with persistent vomiting.
Conclusion: There were no clinically important differences between ORT and IVT in terms of efficacy and safety. For every 25 children (95% CI: 20, 50) treated with ORT, one would fail and require IVT. The results support existing practice guidelines recommending ORT as the first course of treatment in appropriate children with dehydration secondary to gastroenteritis.
Figures
References
-
- American Academy of Pediatrics Provisional committee on quality improvement, subcommittee on acute gastroenteritis, Practice parameter: the management of acute gastroenteritis in young children. Pediatrics. 1996;97:424–35. - PubMed
-
- Armon K, Elliott EJ. Acute gastroenteritis. In: Moyer VA, editor. In Evidence based pediatrics and child health. London: BMJ Books; 2000. pp. 273–86.
-
- World Health Organization (Child and Adolescent Health and Development) Child Health Epidemiology http://www.who.int/child-adolescent-health/overview/child_health/child_e... [Cited 2002 May 6]
-
- World Health Organization The challenge of diarrhoeal and acute respiratory disease control. In Point of Fact No 77 Geneva: World Health Organization. 1996. pp. 1–4.
-
- Duggan C, Santosham M, Glass RI. Centres for Disease Control and Prevention: The management of acute diarrhea in children: oral rehydration, maintenance, and nutritional therapy. MMWR Morbidity and Mortality Weekly Report. 1992;41:1–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
