

Spatial clustering of filarial transmission before and after a Mass Drug Administration in a setting of low infection prevalence
- PMID: 15128461
- PMCID: PMC420477
- DOI: 10.1186/1475-2883-3-3
Spatial clustering of filarial transmission before and after a Mass Drug Administration in a setting of low infection prevalence
Abstract
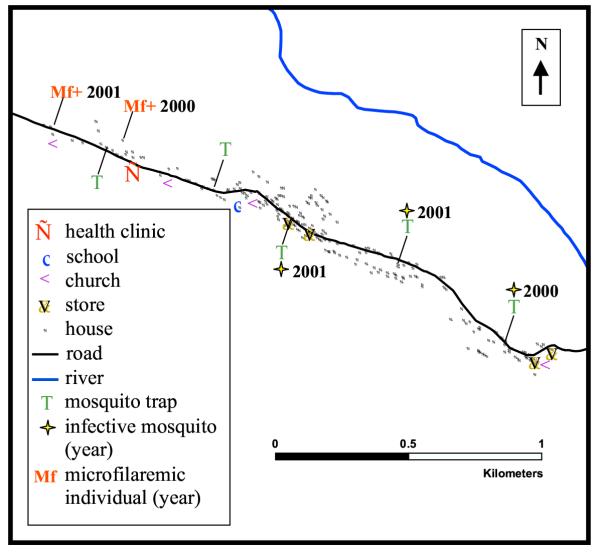
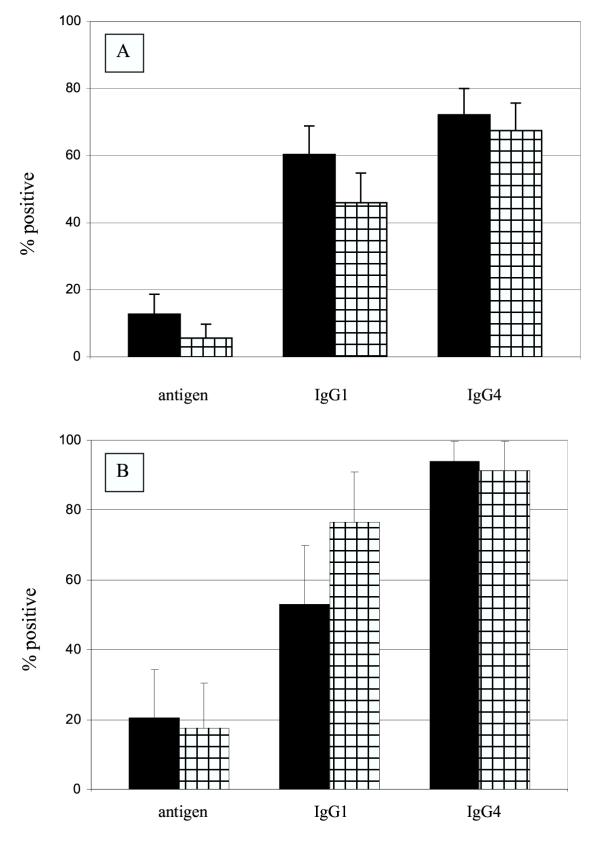
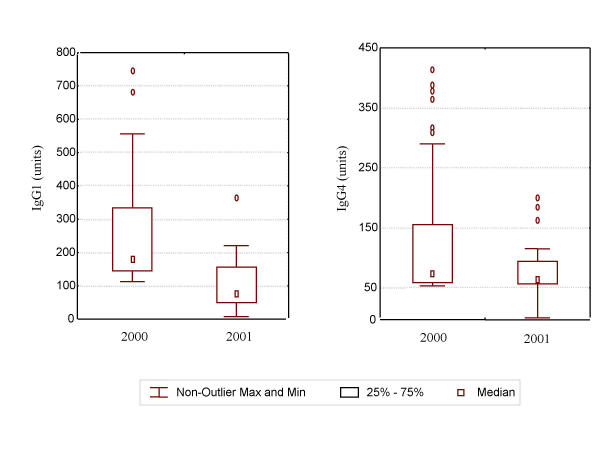
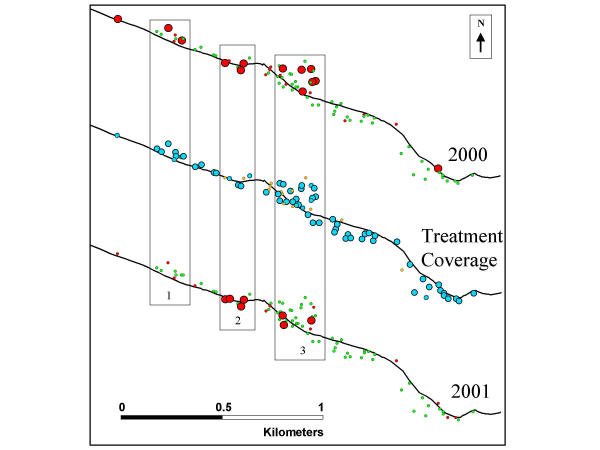
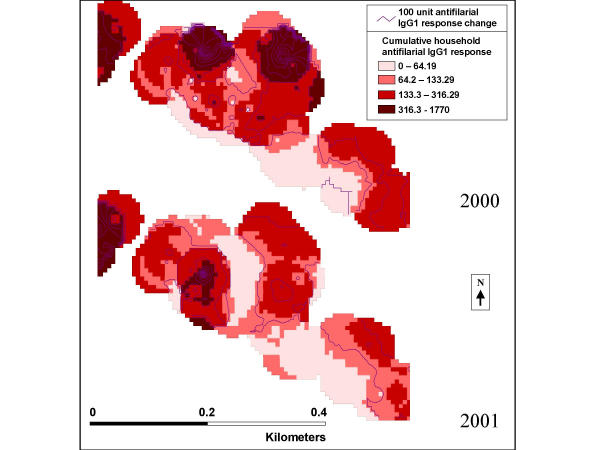
BACKGROUND: In the global program for the elimination of lymphatic filariasis (LF) longitudinal assessment of the prevalence of microfilaremia and antigenemia is recommended to monitor the effect of mass treatment on transmission. Additional monitoring tools such as entomologic and antibody methods may be useful in identifying residual foci of infection. In this study, we characterized serologic markers of infection and exposure spatially both before and after mass treatment, in an area of initial low Wuchereria bancrofti infection prevalence. METHODS: Consenting persons in the sentinel community were tested for circulating microfilaria and antigen (by immunochromatographic test) before and after the 1st annual mass drug administration of diethylcarbamazine and albendazole. A cohort of 161 persons provided serum specimens both years that were tested for antifilarial IgG (1 and 4) antibody. Every house was mapped using a differential Global Positioning System; this information was linked to the serologic data. W. bancrofti infection in the mosquito vector was assessed with year-round collection. Multiple linear regression was used to investigate the influence of antigen-positive persons on the antifilarial antibody responses of antigen-negative neighbors. RESULTS: After mass treatment, decreases were observed in the sentinel site in the overall prevalence of antigen (10.4% to 6.3%) and microfilaremia (0.9 to 0.4%). Of the persons in the cohort that provided serum specimens both years, 79% received treatment. Antigen prevalence decreased from 15.0% to 8.7%. Among 126 persons who received treatment, antigen and antifilarial IgG1 prevalence decreased significantly (p = 0.002 and 0.001, respectively). Among 34 persons who did not receive treatment, antifilarial IgG1 prevalence increased significantly (p = 0.003). Average antifilarial IgG1 levels decreased in households with high treatment coverage and increased in households that refused treatment. Each 10-meter increase in distance from the residence of a person who was antigen-positive in 2000 was associated a 4.68 unit decrease in antifilarial IgG1 level in 2001, controlling for other factors (p = 0.04). DISCUSSION: Antifilarial antibody assays can be used as a measure of filarial exposure. Our results suggest that micro-scale spatial heterogeneity exists in LF exposure and infection. Treatment appeared to be associated with reduced exposure at the sub-community level, suggesting the need to achieve high and homogeneous coverage. Public health messages should note the benefits of having one's neighbors receive treatment with antifilarial drugs.
Figures
References
-
- WHO Lymphatic filariasis. Weekly Epidemiological Record. 2001;76:149–156.
-
- WHO . WHO/CDS/CPE/CEE/200015. Geneva, Switzerland, World Health Organization; 2000. Preparing and implementing a national plan to eliminate lymphatic filariasis.
-
- Lammie PJ, Hightower AW, Eberhard ML. Age-specific prevalence of antigenemia in a Wuchereria bancrofti-exposed population. Am J Trop Med Hyg. 1994;51:348–355. - PubMed
-
- Simonsen PE, Meyrowitsch DW, Jaoko WG, Malecela MN, Mukoko D, Pedersen EM, Ouma JH, Rwegoshora RT, Masese N, Magnussen P, Estambale BB, Michael E. Bancroftian filariasis infection, disease, and specific antibody response patterns in a high and a low endemicity community in East Africa. Am J Trop Med Hyg. 2002;66:550–559. - PubMed
-
- Bockarie MJ, Alexander ND, Hyun P, Dimber Z, Bockarie F, Ibam E, Alpers MP, Kazura JW. Randomised community-based trial of annual single-dose diethylcarbamazine with or without ivermectin against Wuchereria bancrofti infection in human beings and mosquitoes. Lancet. 1998;351:162–168. doi: 10.1016/S0140-6736(97)07081-5. - DOI - PubMed
LinkOut - more resources
Full Text Sources
