

Hematopoietic stem cell transplantation: a primer for the primary care physician
- PMID: 15136552
- PMCID: PMC400723
- DOI: 10.1503/cmaj.1011625
Hematopoietic stem cell transplantation: a primer for the primary care physician
Abstract
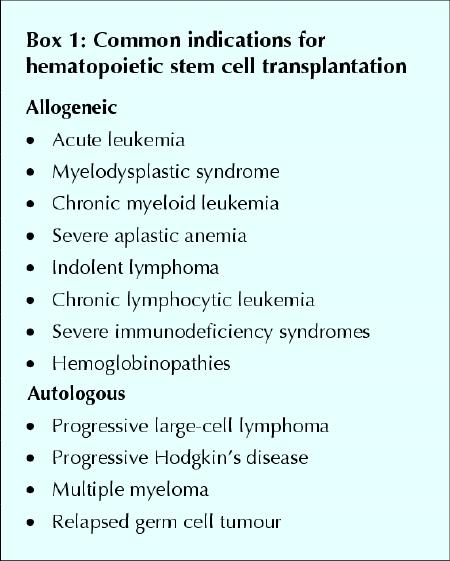
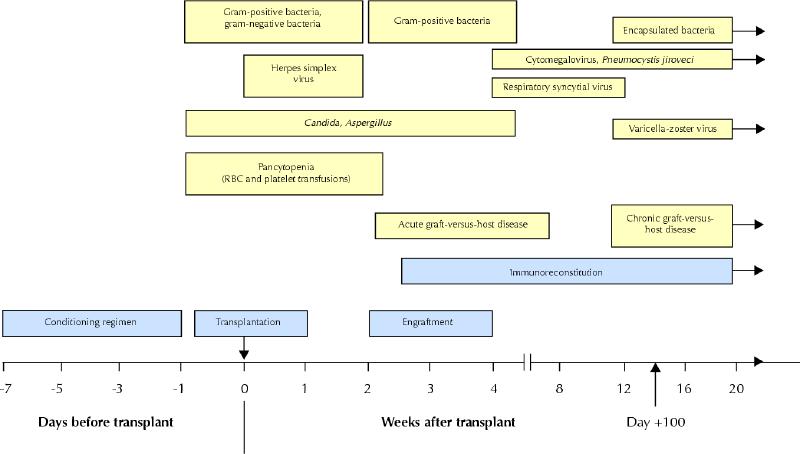
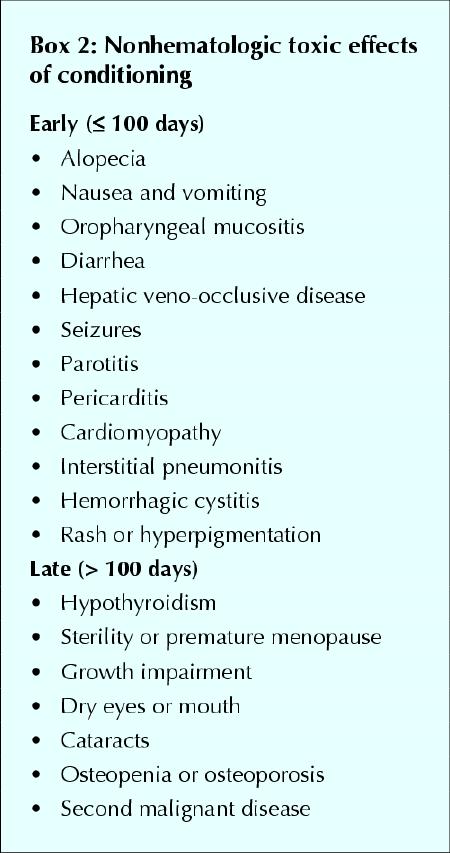
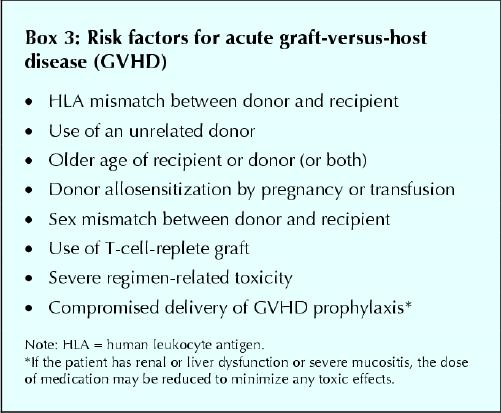
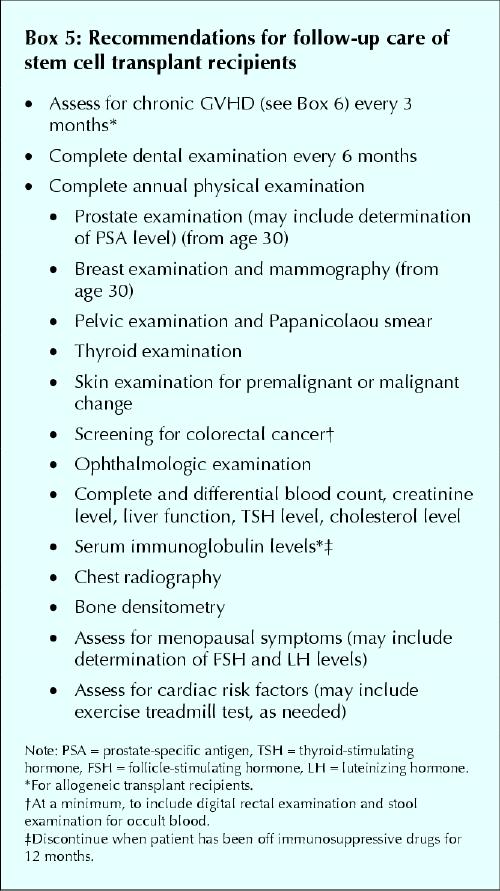
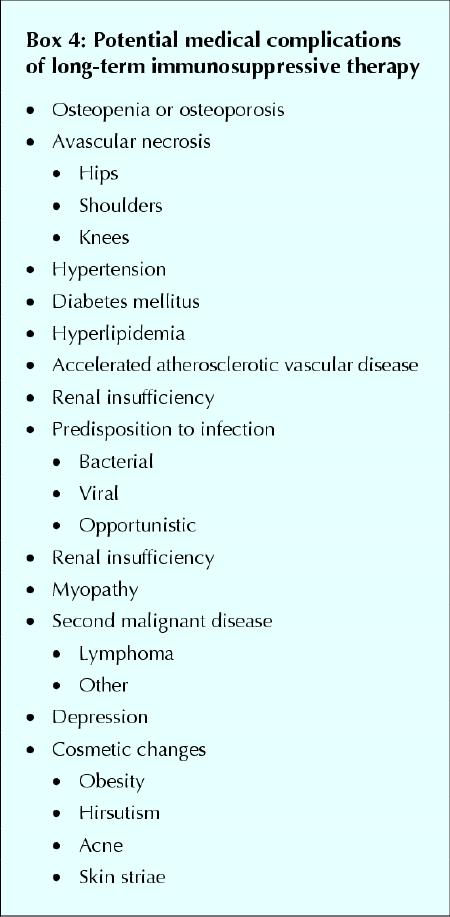
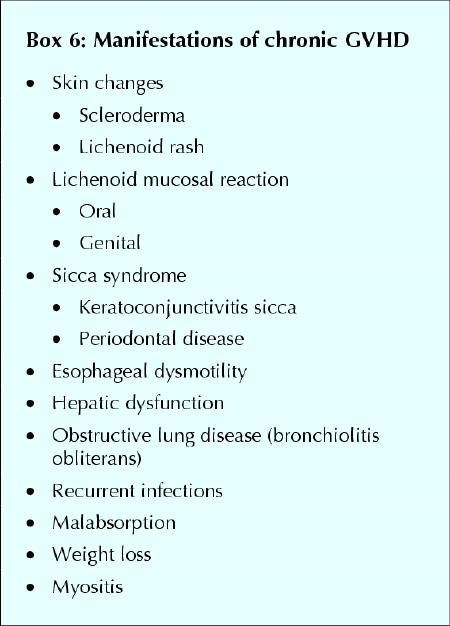
Hematopoietic stem cell transplantation has been used for many years to treat various malignant and nonmalignant hematologic conditions. However, the high-dose conditioning regimen can lead to major organ dysfunction, life-threatening infection and bleeding. In the allogeneic setting, graft-versus-host disease may also develop, making post-transplant management complex. Once a transplant recipient is discharged from hospital and returns to his or her local community, the primary care physician can play an important role in care. Recipients of stem cell transplants may be severely immunocompromised for many months after transplantation, especially if they are still taking immunosuppressive drugs. Furthermore, endocrine and metabolic deficiencies can develop, and transplant survivors are at risk of a second malignant disease. This review is intended as a basic overview of allogeneic and autologous stem cell transplantation with a special focus on long-term follow-up issues relevant to primary care providers.
Figures




Similar articles
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
Second allogeneic stem cell transplantation using nonmyeloablative conditioning for patients who relapsed or developed secondary malignancies following autologous transplantation.Exp Hematol. 2000 Sep;28(9):1096-104. doi: 10.1016/s0301-472x(00)00511-7. Exp Hematol. 2000. PMID: 11008023
-
Epidemiology, management, and outcome of invasive fungal disease in patients undergoing hematopoietic stem cell transplantation in China: a multicenter prospective observational study.Biol Blood Marrow Transplant. 2015 Jun;21(6):1117-26. doi: 10.1016/j.bbmt.2015.03.018. Epub 2015 Mar 31. Biol Blood Marrow Transplant. 2015. PMID: 25840339
-
Favorable impact of natural killer cell reconstitution on chronic graft-versus-host disease and cytomegalovirus reactivation after allogeneic hematopoietic stem cell transplantation.Haematologica. 2014 Dec;99(12):1860-7. doi: 10.3324/haematol.2014.108407. Epub 2014 Aug 1. Haematologica. 2014. PMID: 25085354 Free PMC article.
-
Allogeneic hematopoietic stem cell transplant recipients and parasitic diseases: A review of the literature of clinical cases and perspectives to screen and follow-up active and latent chronic infections.Transpl Infect Dis. 2017 Apr;19(2). doi: 10.1111/tid.12669. Epub 2017 Mar 31. Transpl Infect Dis. 2017. PMID: 28128496 Review.
Cited by
-
Intravenous busulfan: in the conditioning treatment of pediatric patients prior to hematopoietic stem cell transplantation.Paediatr Drugs. 2007;9(4):271-8. doi: 10.2165/00148581-200709040-00008. Paediatr Drugs. 2007. PMID: 17705566
-
The Contemporary Role of Hematopoietic Stem Cell Transplantation in the Management of Chronic Myeloid Leukemia: Is It the Same in All Settings?Cancers (Basel). 2024 Feb 12;16(4):754. doi: 10.3390/cancers16040754. Cancers (Basel). 2024. PMID: 38398145 Free PMC article. Review.
-
Lectins as a promising therapeutic agent for breast cancer: A review.Breast Dis. 2024;43(1):193-211. doi: 10.3233/BD-230047. Breast Dis. 2024. PMID: 38905027 Free PMC article. Review.
-
Medication Adherence in Patients with Hematologic Malignancies Who Are Hematopoietic Stem Cell Transplantation Survivors: A Qualitative Study.Transplant Cell Ther. 2023 Oct;29(10):620.e1-620.e11. doi: 10.1016/j.jtct.2023.07.019. Epub 2023 Jul 27. Transplant Cell Ther. 2023. PMID: 37516379 Free PMC article.
-
Intravenous busulfan: a guide to its use as conditioning treatment before transplantation of haematopoietic progenitor cells.Clin Drug Investig. 2012 Sep 1;32(9):641-8. doi: 10.1007/BF03261918. Clin Drug Investig. 2012. PMID: 22877323
References
-
- Santos GW. Bone marrow transplantation. In: Stollerman GH, editor. Advances in internal medicine. Chicago: Year Book Publishers; 1975. p. 157-82. - PubMed
-
- Lorenz E, Uphoff DE, Reid TR, Shelton E. Modification of acute irradiation injury in mice and guinea pigs by bone marrow injection. Radiology 1951; 58: 863-77. - PubMed
-
- Cohen JA, Vos O, van Bekkum DW. The present status of radiation protection by chemical and biological agents in mammals. In: de Hevesy GC, Forssberg AG, Abbott JD, editors. Advances in radiobiology. Edinburgh: Oliver and Boyd; 1957. p. 134-44.
-
- Billingham RE. The biology of graft-versus-host reactions. Harvey Lect 1966-67;62:21-78. - PubMed
-
- Bearman SI, Mori M, Beatty PG, Meyer WG, Buckner CD, Petersen FB, et al. Comparison of morbidity and mortality after marrow transplantation from HLA-genotypically identical siblings and HLA-phenotypically identical unrelated donors. Bone Marrow Transplant 1994;13(1):31-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources