

Comparison of cerebral blood volume and vascular permeability from dynamic susceptibility contrast-enhanced perfusion MR imaging with glioma grade
- PMID: 15140713
- PMCID: PMC7974484
Comparison of cerebral blood volume and vascular permeability from dynamic susceptibility contrast-enhanced perfusion MR imaging with glioma grade
Abstract
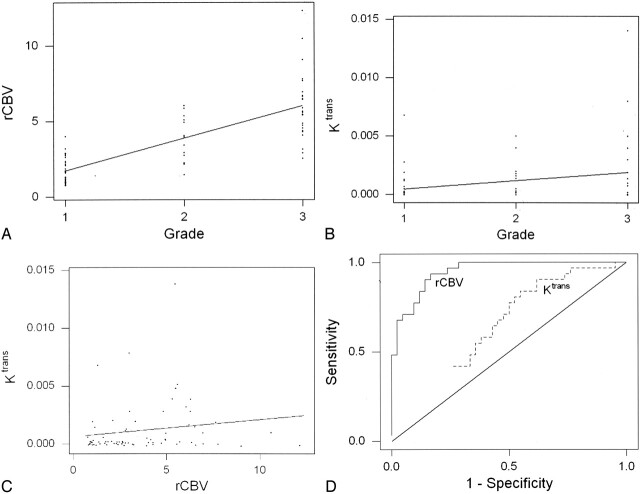
Background and purpose: Relative cerebral blood volume (rCBV) and vascular permeability (K(trans)) permit in vivo assessment of glioma microvasculature. We assessed the associations between rCBV and K(trans) derived from dynamic, susceptibility-weighted, contrast-enhanced (DSC) MR imaging and tumor grade and between rCBV and K(trans).
Methods: Seventy-three patients with primary gliomas underwent conventional and DSC MR imaging. rCBVs were obtained from regions of maximal abnormality for each lesion on rCBV color maps. K(trans) was derived from a pharmacokinetic modeling algorithm. Histopathologic grade was compared with rCBV and K(trans) (Tukey honestly significant difference). Spearman and Pearson correlation factors were determined between rCBV, K(trans), and tumor grade. The diagnostic utility of rCBV and K(trans) in discriminating grade II or III tumors from grade I tumors was assessed by logistic regression.
Results: rCBV was significantly different for all three grades (P </=.0005). K(trans) was significantly different between grade I and grade II or III (P =.027) but not between other grades or combinations of grades. Spearman rank and Pearson correlations, respectively, were as follows: rCBV and grade, r = 0.817 and r = 0.771; K(trans) and grade, r = 0.234 and r = 0.277; and rCBV and K(trans), r = 0.266 and r = 0.163. Only rCBV was significantly predictive of high-grade gliomas (P <.0001).
Conclusion: rCBV with strongly correlated with tumor grade; the correlation between K(trans) and tumor grade was weaker. rCBV and K(trans) were positively but weakly correlated, suggesting that these parameters demonstrate different tumor characteristics. rCBV is a more significant predictor of high-grade glioma than K(trans).
Figures
Comment in
-
What is right about MRI permeability studies.AJNR Am J Neuroradiol. 2005 Jan;26(1):3-4. AJNR Am J Neuroradiol. 2005. PMID: 15661689 Free PMC article. No abstract available.
References
-
- Daumas-Duport C, Scheithauer B, O’Fallon J, Kelly P. Grading of astrocytomas: a simple and reproducible method. Cancer 1988;62:2152–2165 - PubMed
-
- Christoforidis GA, Bourekas EC, Baujan M, et al. High resolution MRI of the deep brain vascular anatomy at 8 tesla: susceptibility-based enhancement of the venous structures. J Comput Assist Tomogr 1999;23:857–866 - PubMed
-
- Burger P. Malignant astrocytic neoplasms: classification, pathology, anatomy, and response to therapy. Semin Oncol 1986;13:16–20 - PubMed
-
- Aronen HJ, Gazit IE, Louis DN, et al. Cerebral blood volume maps of gliomas: comparison with tumor grade and histologic findings. Radiology 1994;191:41–51 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical