

Swimmer's CT: improved imaging of the lower neck and thoracic inlet
Affiliations
- PMID: 15140736
- PMCID: PMC7974463
Item in Clipboard
Swimmer's CT: improved imaging of the lower neck and thoracic inlet
AJNR Am J Neuroradiol.
2004 May.
Abstract
CT findings of the base of the neck are often degraded by beam-hardening artifact from the shoulder girdle. This artifact can be reduced by placing the patient in a "swimmer's" position, a supine position in which the patient has one arm fully abducted and the other arm lowered. We selectively employed swimmer's CT in patients between January 1999 and December 2002 when standard (arms-down) CT failed to depict suspected disease. In nine of 10 patients, swimmer's CT improved CT quality or accuracy or both over that obtained when the standard CT position was used.
Figures
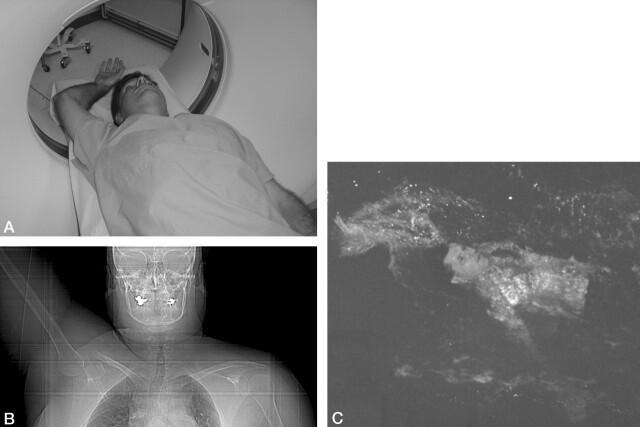
A, Volunteer in swimmer’s position, with one arm raised above head, the other with shoulder depressed, while supine within CT scanner. B, CT scout in swimmer’s position. Note the right humoral head and clavicle are no longer in the same axial plane as the left. C, Backstroke while swimming, from which the swimmer’s position is named.

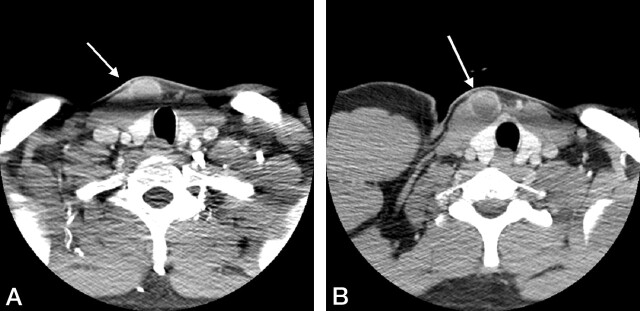
A, In normal position, beam hardening completely obscures pretracheal soft tissues (open arrow). B, With swimmer’s positioning, the arrow depicts a pretracheal lymph node just above the thyroid isthmus, and just beneath the larynx. This node has been referred to as the Delphian node and is not visible in the left image because of artifact. Notice the asymmetry of the clavicle and scapular position and musculature in the swimmer’s position (B), making normal anatomy more difficult to assess. This later point constitutes cause for reservation of the swimmer’s position until after normal anatomy has been initially assessed with conventional (symmetric) positioning.
A, Beam hardening at the level of the thyroid isthmus results in decreased soft-tissue contrast and obscures the vascular malformation (arrow) anterior to the right sternocledomastoid muscle, which is better seen in panel B, with the swimmer’s position (open arrow). This lesion had been present and stable for many years and may actually represent a type II or III branchial cleft cyst, as it lies anterior to the lowermost aspect of the sternocleidomastoid muscle. No tract was visible; thus, venous or lymphatic malformation was the favored diagnosis.

Seat-belt deceleration vertical fracture of anterior aspect of second thoracic (T2) vertebral body. Multidetector CT in standard (A and C) and swimmer’s (B and D) position obtained by reformatted 0.6-mm-thick axial images then sagittally reconstructed. The superior mediastinum and soft tissues are more distinct in panel B than in panel A, whereas swimmer’s sagittal reconstruction (D) more sharply demarcates the fracture boundary and endplate defects (arrow). E, Proton density-weighted sagittal MR confirms the lower T2 endplate defect (arrow). F, Fat-suppressed T2-weighted sagittal MR confirms acuity of fracture on the basis of marrow edema (arrow).

Right C7 radiculopathy evaluated with cervical postmyelography CT axial images at 1.5-mm thickness at same level in standard (A) and swimmer’s (B) position. A, Beam hardening produces linear areas of decreased attenuation in the right foramen, contrast-opacified CSF and spinal cord, and linear variable attenuation in the left foramen and soft tissues compared with swimmer’s CT (B) B, Swimmer’s CT demonstrates distinct uniform soft-tissue attenuation representing formamenal disk herniation (surgically confirmed) in the right foramen (arrows) while also better demonstrating normal uniform fat attenuation surrounding the nerve root sleeve in the normal left foramen.
References
-
- Gisbert VL, Hollerman JJ, Ney AL, et al. Incidence and diagnosis of C7–T1 fractures and subluxations in multiple-trauma patients: evaluation of the advanced trauma life support guidelines. Surgery 1989;106:702–708 - PubMed
-
- Advanced trauma life support. Committee on Trauma, American College of Surgeons. Paul E (chairman), ed.1984;7:128
-
- Tehranzadeh J, Bonk RT, Ansari A, Mesgarzadeh M. Efficacy of limited CT for nonvisualized lower cervical spine in patients with blunt trauma. Skeletal Radiol 1994;23:349–352 - PubMed
-
- Bilbey JH, Muller NL, Connell DG, et al. Thoracic outlet syndrome: evaluation with CT. Radiology 1989;171:381–384. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical