

Eosinophilia in a patient with cyclical vomiting: a case report
- PMID: 15144561
- PMCID: PMC425596
- DOI: 10.1186/1476-7961-2-7
Eosinophilia in a patient with cyclical vomiting: a case report
Abstract
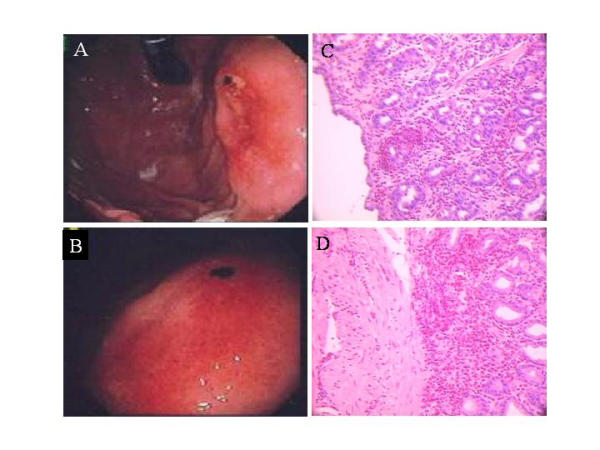
BACKGROUND: Eosinophilic gastritis is related to eosinophilic gastroenteritis, varying only in regards to the extent of disease and small bowel involvement. Common symptoms reported are similar to our patient's including: abdominal pain, epigastric pain, anorexia, bloating, weight loss, diarrhea, ankle edema, dysphagia, melaena and postprandial nausea and vomiting. Microscopic features of eosinophilic infiltration usually occur in the lamina propria or submucosa with perivascular aggregates. The disease is likely mediated by eosinophils activated by various cytokines and chemokines. Therapy centers around the use of immunosuppressive agents and dietary therapy if food allergy is a factor. CASE PRESENTATION: The patient is a 31 year old Caucasian female with a past medical history significant for ulcerative colitis. She presented with recurrent bouts of vomiting, abdominal pain and chest discomfort of 11 months duration. The bouts of vomiting had been reoccurring every 7-10 days, with each episode lasting for 1-3 days. This was associated with extreme weakness and cachexia. Gastric biopsies revealed intense eosinophilic infiltration. The patient responded to glucocorticoids and azathioprine. The differential diagnosis and molecular pathogenesis of eosinophilic gastritis as well as the molecular effects of glucocorticoids in eosinophilic disorders are discussed. CONCLUSIONS: The patient responded to a combination of glucocorticosteroids and azathioprine with decreased eosinophilia and symptoms. It is likely that eosinophil-active cytokines such as interleukin-3 (IL-3), granulocyte macrophage colony stimulating factor (GM-CSF) and IL-5 play pivotal roles in this disease. Chemokines such as eotaxin may be involved in eosinophil recruitment. These mediators are downregulated or inhibited by the use of immunosuppressive medications.
Figures


References
-
- Robinson J, Ahmed Z, Siddiqui A, Roy T, Berk S, Smith JK, Krishnaswamy G. A patient with persistent wheezing, sinusitis, elevated IgE, and eosinophilia. Ann Allergy Asthma Immunol. 1999;82:144–149. - PubMed
-
- Brenner MA, Patel MB. Cutaneous larva migrans: the creeping eruption. Cutis. 2003;72:111–115. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
