

Influence of human T lymphotrophic virus type I on diffuse pan-bronchiolitis
- PMID: 15147354
- PMCID: PMC1809062
- DOI: 10.1111/j.1365-2249.2004.02485.x
Influence of human T lymphotrophic virus type I on diffuse pan-bronchiolitis
Abstract
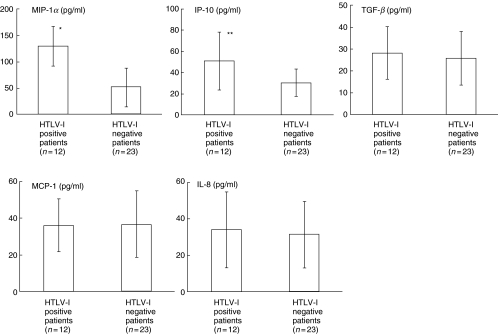
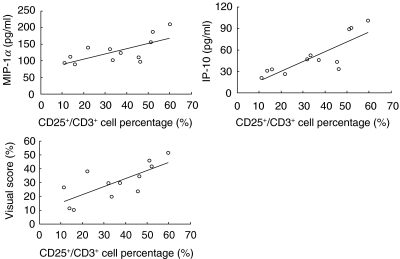
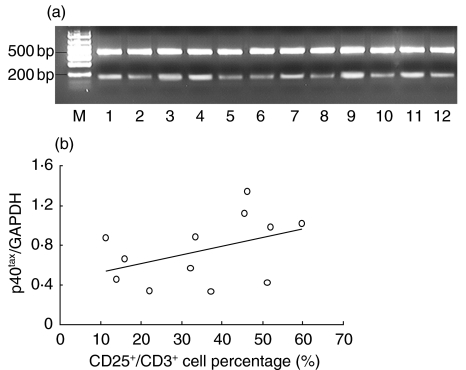
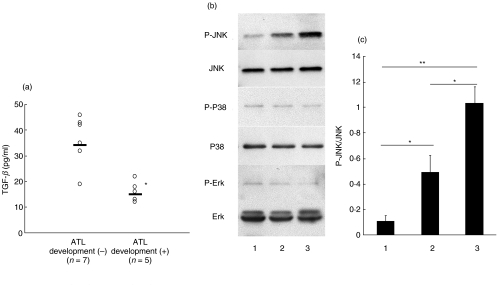
Human T lymphotrophic virus type-I (HTLV-I), a human retrovirus, infects CD4(+) lymphocytes and is thought to modify their function and a possible association with pulmonary diseases has also been suggested. However, little is known about the influence of HTLV-I on diffuse pan-bronchiolitis (DPB), a chronic inflammatory lung disease with infiltration of lymphocytes and hyperplasia of the bronchus-associated lymphoid tissue. In this study, 35 DPB patients with and without HTLV-I infection were examined. HTLV-I positive DPB patients were likely to have a larger affected area with lower FEV(1). The CD3(+)/CD25(+) lymphocyte percentage was significantly higher in the BALF of HTLV-I positive patients than in negative patients. MIP-1 alpha, IP-10 and levels in BALF were also significantly higher in HTLV-I positive patients than in negative patients. The levels of MCP-1 and IL-8 were not significantly different. In HTLV-I positive patients, the MIP-1 alpha and IP-10 levels showed a significant positive correlation with the percentage of CD3(+)/CD25 lymphocytes. BALF cells of all HTLV-I positive DPB patients showed expression of p40(tax) mRNA. We suggest that HTLV-I infection may modify DPB pathogenesis via activation of T cells. We also found that the frequency of ATL development in HTLV-I positive DPB patients was significantly higher than in all HTLV-I positive patients (OR = 8.22, 95% CI = 2.61-25.9, P < 0.01). The levels of TGF-beta in patients who developed ATL were significantly lower than in patients who did not develop ATL. Sensitivity and specificity were 80% and 85.7%, respectively (cut-off = 20 pg/ml). We also propose that these features should be taken into consideration in the treatment of DPB in HTLV-I infected individuals.
Figures
Similar articles
-
Influence of human T lymphotrophic virus type I on cryptogenic fibrosing alveolitis - HTLV-I associated fibrosing alveolitis: proposal of a new clinical entity.Clin Exp Immunol. 2003 Sep;133(3):397-403. doi: 10.1046/j.1365-2249.2003.02240.x. Clin Exp Immunol. 2003. PMID: 12930367 Free PMC article.
-
[Association between diffuse panbronchiolitis and HTLV-I infection].Nihon Kyobu Shikkan Gakkai Zasshi. 1994 Jan;32(1):17-24. Nihon Kyobu Shikkan Gakkai Zasshi. 1994. PMID: 8114368 Japanese.
-
Elevated levels of beta-chemokines in bronchoalveolar lavage fluid (BALF) of individuals infected with human T lymphotropic virus type-1 (HTLV-1).Clin Exp Immunol. 1999 Dec;118(3):417-22. doi: 10.1046/j.1365-2249.1999.01093.x. Clin Exp Immunol. 1999. PMID: 10594561 Free PMC article.
-
Virological and immunological mechanisms in the pathogenesis of human T-cell leukemia virus type 1.Rev Med Virol. 2013 Sep;23(5):269-80. doi: 10.1002/rmv.1745. Epub 2013 Apr 22. Rev Med Virol. 2013. PMID: 23606621 Review.
-
HTLV-1 infection: what determines the risk of inflammatory disease?Trends Microbiol. 2012 Oct;20(10):494-500. doi: 10.1016/j.tim.2012.07.004. Epub 2012 Aug 21. Trends Microbiol. 2012. PMID: 22917680 Review.
Cited by
-
CT Chest and pulmonary functional changes in patients with HTLV-associated myelopathy in the Eastern Brazilian Amazon.PLoS One. 2017 Nov 2;12(11):e0186055. doi: 10.1371/journal.pone.0186055. eCollection 2017. PLoS One. 2017. PMID: 29095831 Free PMC article.
-
Human T-cell leukaemia virus type 1 associated pulmonary disease: clinical and pathological features of an under-recognised complication of HTLV-1 infection.Retrovirology. 2021 Jan 6;18(1):1. doi: 10.1186/s12977-020-00543-z. Retrovirology. 2021. PMID: 33407607 Free PMC article. Review.
-
Human T Lymphotropic Virus and Pulmonary Diseases.Front Microbiol. 2018 Aug 14;9:1879. doi: 10.3389/fmicb.2018.01879. eCollection 2018. Front Microbiol. 2018. PMID: 30154781 Free PMC article. Review.
-
The Role of Chemokines in the Pathogenesis of HTLV-1.Front Microbiol. 2020 Mar 13;11:421. doi: 10.3389/fmicb.2020.00421. eCollection 2020. Front Microbiol. 2020. PMID: 32231656 Free PMC article. Review.
-
An Overview of Human T-Lymphotropic Virus Type 1 Lung Injury.Front Immunol. 2022 Jul 1;13:914498. doi: 10.3389/fimmu.2022.914498. eCollection 2022. Front Immunol. 2022. PMID: 35844492 Free PMC article. Review.
References
-
- Homma H, Yamanaka A, Tanimoto S, et al. Diffuse panbronchiolitis. A disease of the transitional zone of the lung. Chest. 1983;83:63–9. - PubMed
-
- Sato A, Chida K, Iwata M, Hayakawa H. Study of bronchus-associated lymphoid tissue in patients with diffuse panbronchiolitis. Am Rev Respir Dis. 1992;146:473–8. - PubMed
-
- Mukae H, Kadota J, Kohno S, et al. Increase in activated CD8+ cells in bronchoalveolar lavage fluid in patients with diffuse panbronchiolitis. Am J Respir Crit Care Med. 1995;152:613–8. - PubMed
-
- Blayney DW, Blattner WA, Jaffe ES, Gallo RC. Retroviruses in human leukemia. Hematol Oncol. 1983;1:193–204. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
