

Survival results of a multicentre phase II study to evaluate D2 gastrectomy for gastric cancer
- PMID: 15150592
- PMCID: PMC2409745
- DOI: 10.1038/sj.bjc.6601761
Survival results of a multicentre phase II study to evaluate D2 gastrectomy for gastric cancer
Abstract
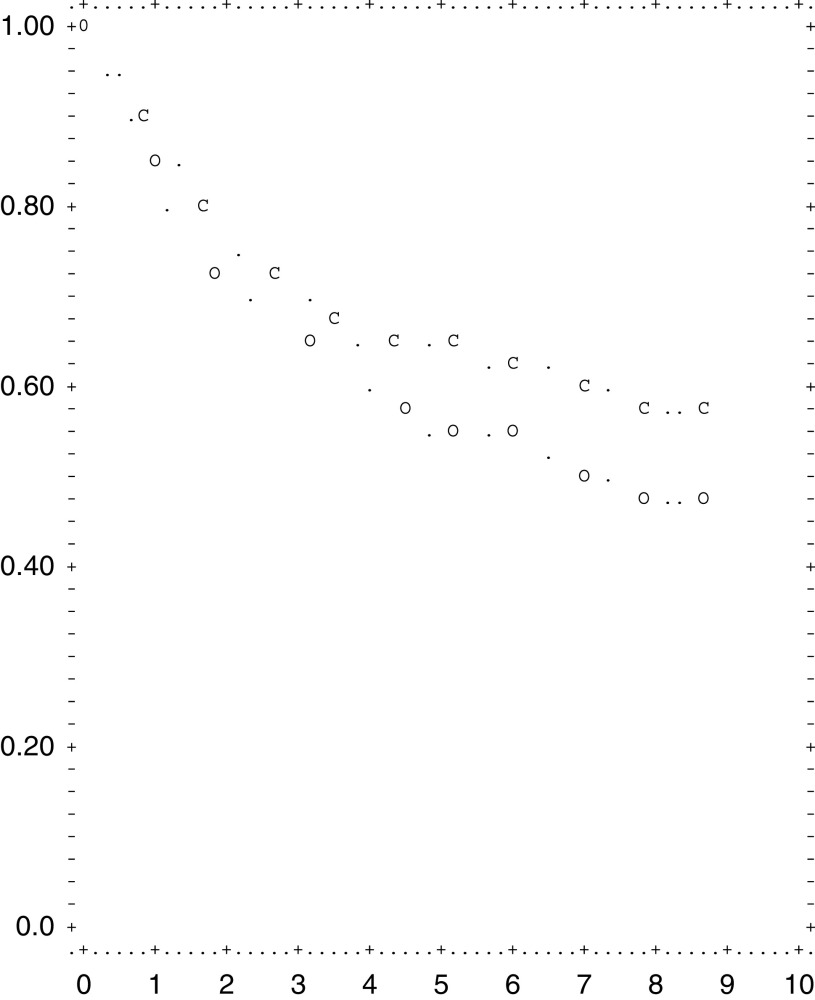
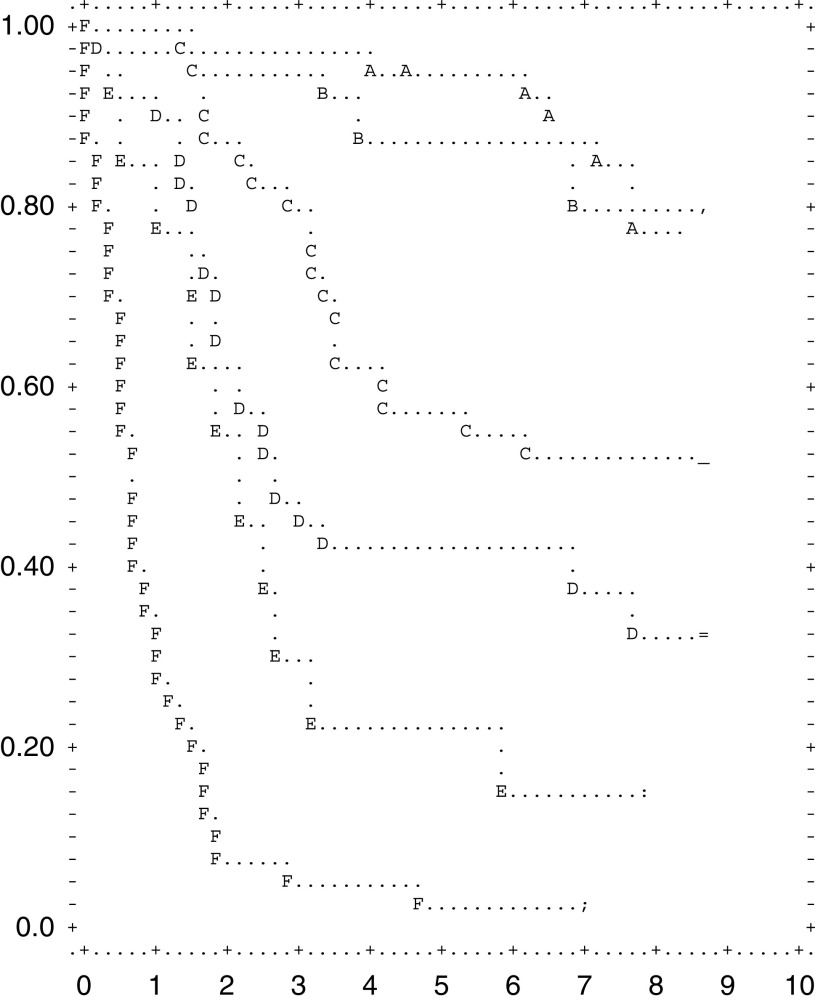
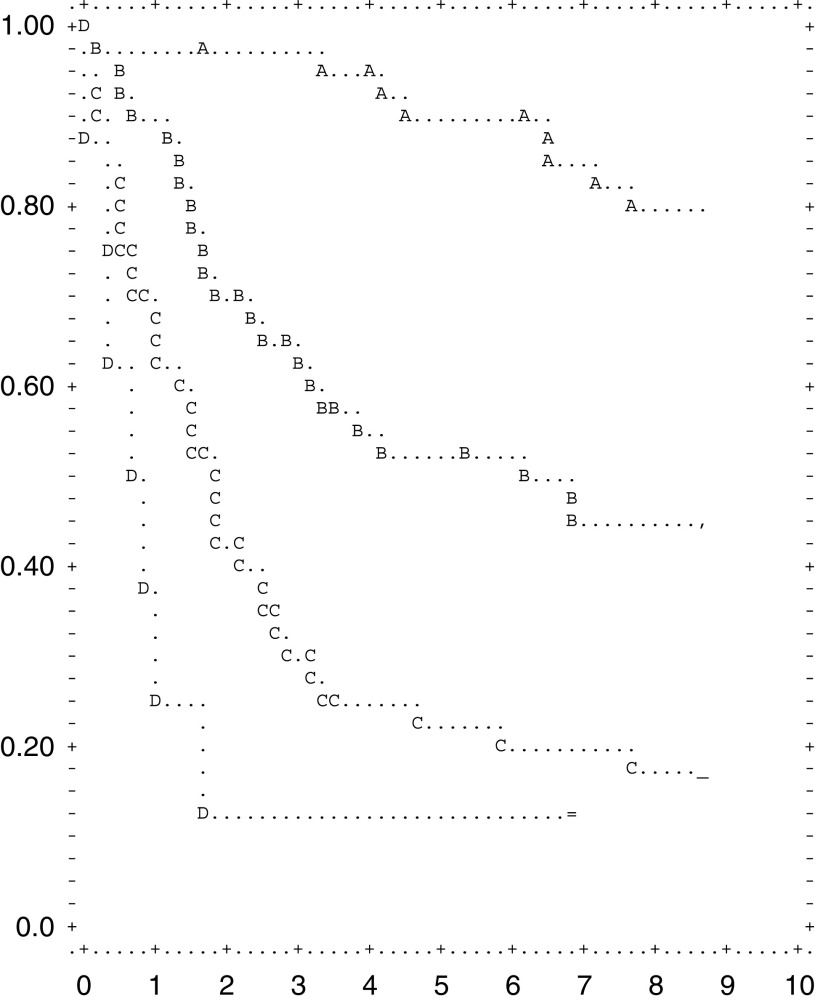
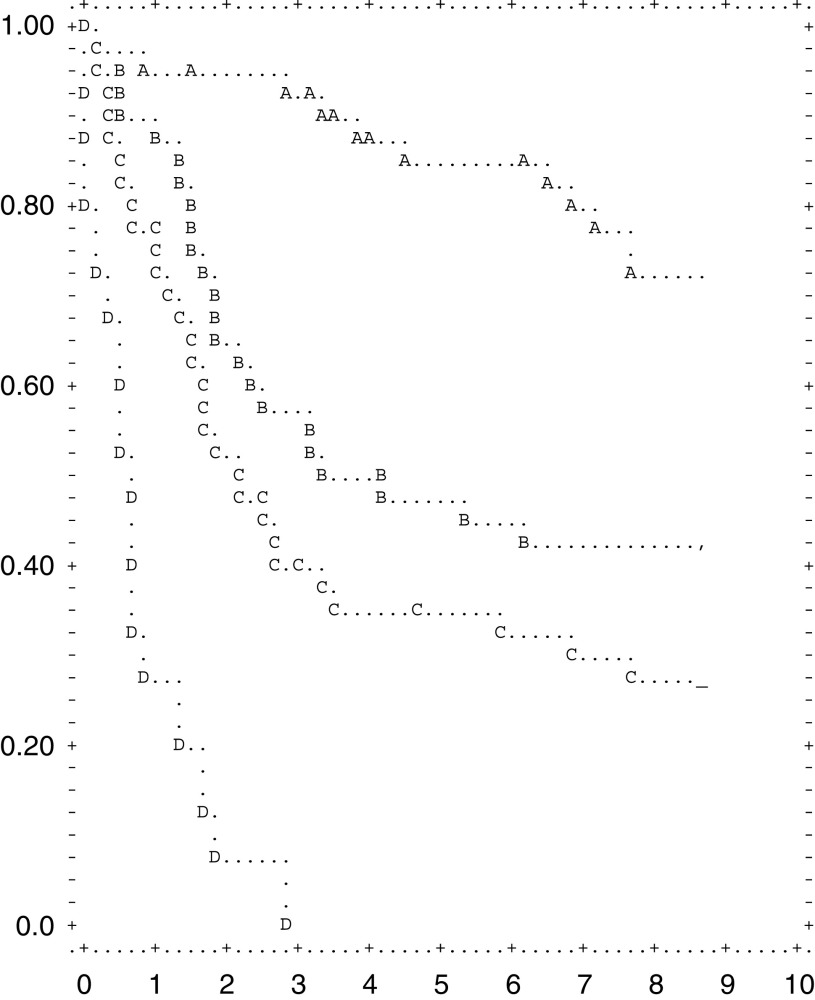
Curative resection is the treatment of choice for potentially curable gastric cancer. Two major Western studies in the 1990s failed to show a benefit from D2 dissection. They showed extremely high postoperative mortality after D2 dissection, and were criticised for the potential inadequacy of the pretrial training in the new technique of D2 dissection, prior to the phase III studies being initiated. The inclusion of pancreatectomy and splenectomy in D2 dissection was associated with increased morbidity and mortality. Following these results, we started a phase II trial to evaluate the safety and efficacy of pancreas-preserving D2 dissection. The results of this trial regarding the safety of pancreas preserving D2 dissection were published in 1998. In this paper, we present the survival results of this phase II trial to confirm the rationale of carrying out a phase III study comparing D1 vs D2 dissection for curable gastric cancer. Italian patients with histologically proven gastric adenocarcinoma were registered in the Italian Gastric Cancer Study Group Multicenter trial. The study was carried out based on the General Rules of the Japanese Research Society for Gastric Cancer. A strict quality control system was achieved by a supervising surgeon of the reference centre who had stayed at the National Cancer Center Hospital, Tokyo, to learn the standard D2 gastrectomy and the postoperative management. The standard procedure entailed removal of the first and second tier lymph nodes. During total gastrectomy, the pancreas was preserved according to the Maruyama technique. Complete follow-up was available to death or 5 years in 100% of patients and the median follow-up time was 4.38 years. Out of 297 consecutive patients registered, 191 patients were enrolled in the study between May 1994 and December 1996. The overall morbidity rate was 20.9%. The postoperative in-hospital mortality was 3.1%. The overall 5-year survival rate among all eligible patients was 55%. Survival was strictly related to stage, depth of wall invasion, lymph node involvement and type of gastrectomy (distal vs total). Our results suggest a survival benefit for pancreas-preserving D2 dissection in Italian patients with gastric cancer if performed in experienced centres. A phase III trial among exclusively experienced centres is urgently needed.
Figures
References
-
- Altorki NK, Skinner DB (1997) Occult cervical nodal metastasis in esophageal cancer: preliminary results of three-field lymphadenectomy. J Thorac Cardiovas Surg 113: 540–544 - PubMed
-
- Bonenkamp JJ, Hermans J, Sasako M, Van De Velde CJH, for the Dutch Gastric Cancer Group (1999) Extended lymph-node dissection for gastric cancer. N Engl J Med 340: 908–914 - PubMed
-
- Bonenkamp JJ, Songun I, Welvaart K, van de Velde CJH, Hermans J, Sasako M, Plukker JTM, van Elk P, Obertop H, Gouma DJ, Taat CW, van Lanschot J, Meyer S, de Graaf PW, von Meyenfeldt MF, Tilanus H (1995) Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet 345: 745–748 - PubMed
-
- Bottger TC, Junginger T (1999) Factors influencing morbidity and mortality after pancreaticoduodenectomy: critical analysis of 221 resections. World J Surg 23: 164–171 - PubMed
-
- Cuschieri A, Fayers P, Fielding J, Craven J, Bancewicz J, Joypaul V, Cook P (1996) Postoperative morbidity and mortality after R1 and R2 resection for gastric cancer: results of the MRC surgical trial. Lancet 347: 995–999 - PubMed
