

Hyperglycaemic index as a tool to assess glucose control: a retrospective study
- PMID: 15153239
- PMCID: PMC468891
- DOI: 10.1186/cc2840
Hyperglycaemic index as a tool to assess glucose control: a retrospective study
Abstract
Introduction: Critically ill patients may benefit from strict glucose control. An objective measure of hyperglycaemia for assessing glucose control in acutely ill patients should reflect the magnitude and duration of hyperglycaemia, should be independent of the number of measurements, and should not be falsely lowered by hypoglycaemic values. The time average of glucose values above the normal range meets these requirements.
Methods: A retrospective, single-centre study was performed at a 12-bed surgical intensive care unit. From 1990 through 2001 all patients over 15 years, staying at least 4 days, were included. Admission type, sex, age, Acute Physiology and Chronic Health Evaluation II score and outcome were recorded. The hyperglycaemic index (HGI) was defined as the area under the curve above the upper limit of normal (glucose level 6.0 mmol/l) divided by the total length of stay. HGI, admission glucose, mean morning glucose, mean glucose and maximal glucose were calculated for each patient. The relations between these measures and 30-day mortality were determined.
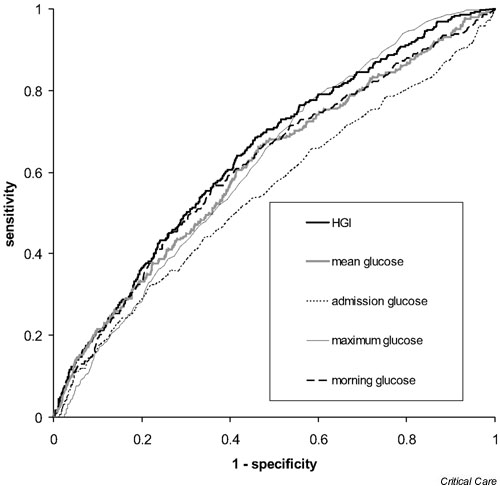
Results: In 1779 patients with a median stay in the intensive care unit of 10 days, the 30-day mortality was 17%. A total of 65,528 glucose values were analyzed. Median HGI was 0.9 mmol/l (interquartile range 0.3-2.1 mmol/l) in survivors versus 1.8 mmol/l (interquartile range 0.7-3.4 mmol/l) in nonsurvivors (P < 0.001). The area under the receiver operator characteristic curve was 0.64 for HGI, as compared with 0.61 and 0.62 for mean morning glucose and mean glucose. HGI was the only significant glucose measure in binary logistic regression.
Conclusion: HGI exhibited a better relation with outcome than other glucose indices. HGI is a useful measure of glucose control in critically ill patients.
Figures



Comment in
-
How to compare adequacy of algorithms to control blood glucose in the intensive care unit?Crit Care. 2004 Jun;8(3):151-2. doi: 10.1186/cc2856. Epub 2004 Mar 23. Crit Care. 2004. PMID: 15153231 Free PMC article.
Similar articles
-
How to compare adequacy of algorithms to control blood glucose in the intensive care unit?Crit Care. 2004 Jun;8(3):151-2. doi: 10.1186/cc2856. Epub 2004 Mar 23. Crit Care. 2004. PMID: 15153231 Free PMC article.
-
[The association between early blood glucose fluctuation and prognosis in critically ill patients].Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2012 Jan;24(1):50-3. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2012. PMID: 22248753 Chinese.
-
Implementation and evaluation of the SPRINT protocol for tight glycaemic control in critically ill patients: a clinical practice change.Crit Care. 2008;12(2):R49. doi: 10.1186/cc6868. Epub 2008 Apr 16. Crit Care. 2008. PMID: 18412978 Free PMC article.
-
Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients.Mayo Clin Proc. 2003 Dec;78(12):1471-8. doi: 10.4065/78.12.1471. Mayo Clin Proc. 2003. PMID: 14661676
-
Glucose control in the intensive care unit.Crit Care Med. 2009 May;37(5):1769-76. doi: 10.1097/CCM.0b013e3181a19ceb. Crit Care Med. 2009. PMID: 19325461 Review.
Cited by
-
Impact of retrospective calibration algorithms on hypoglycemia detection in newborn infants using continuous glucose monitoring.Diabetes Technol Ther. 2012 Oct;14(10):883-90. doi: 10.1089/dia.2012.0111. Epub 2012 Aug 2. Diabetes Technol Ther. 2012. PMID: 22856622 Free PMC article.
-
Stress-Induced and Diabetic Hyperglycemia Associated with Higher Mortality among Intensive Care Unit Trauma Patients: Cross-Sectional Analysis of the Propensity Score-Matched Population.Int J Environ Res Public Health. 2018 May 15;15(5):992. doi: 10.3390/ijerph15050992. Int J Environ Res Public Health. 2018. PMID: 29762485 Free PMC article.
-
A stepwise approach toward closed-loop blood glucose control for intensive care unit patients: results from a feasibility study in type 1 diabetic subjects using vascular microdialysis with infrared spectrometry and a model predictive control algorithm.J Diabetes Sci Technol. 2011 Jul 1;5(4):901-5. doi: 10.1177/193229681100500412. J Diabetes Sci Technol. 2011. PMID: 21880232 Free PMC article. Clinical Trial.
-
Relationship of hyperglycemia and surgical-site infection in orthopaedic surgery.J Bone Joint Surg Am. 2012 Jul 3;94(13):1181-6. doi: 10.2106/JBJS.K.00193. J Bone Joint Surg Am. 2012. PMID: 22760385 Free PMC article.
-
How to compare adequacy of algorithms to control blood glucose in the intensive care unit?Crit Care. 2004 Jun;8(3):151-2. doi: 10.1186/cc2856. Epub 2004 Mar 23. Crit Care. 2004. PMID: 15153231 Free PMC article.
References
-
- Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426–2432. - PubMed
-
- van den Berghe G, Wouters PJ, Bouillon R, Weekers F, Verwaest C, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P. Outcome benefit of intensive insulin therapy in the critically ill: Insulin dose versus glycemic control. Crit Care Med. 2003;31:359–366. doi: 10.1097/01.CCM.0000045568.12881.10. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
