

Home based therapy for severe malnutrition with ready-to-use food
- PMID: 15155403
- PMCID: PMC1719944
- DOI: 10.1136/adc.2003.034306
Home based therapy for severe malnutrition with ready-to-use food
Abstract
Background: The standard treatment of severe malnutrition in Malawi often utilises prolonged inpatient care, and after discharge results in high rates of relapse.
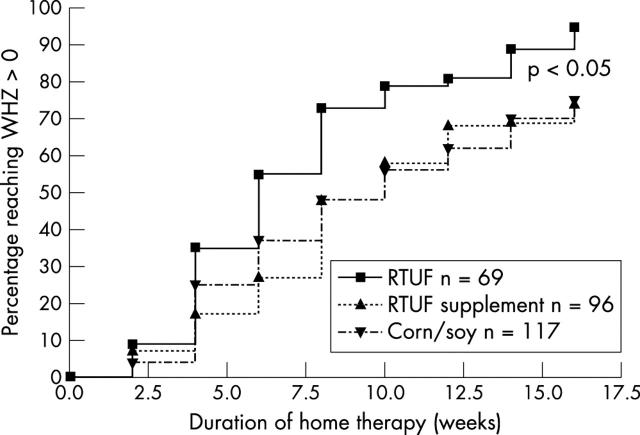
Aims: To test the hypothesis that the recovery rate, defined as catch-up growth such that weight-for-height z score >0 (WHZ, based on initial height) for ready-to-use food (RTUF) is greater than two other home based dietary regimens in the treatment of malnutrition.
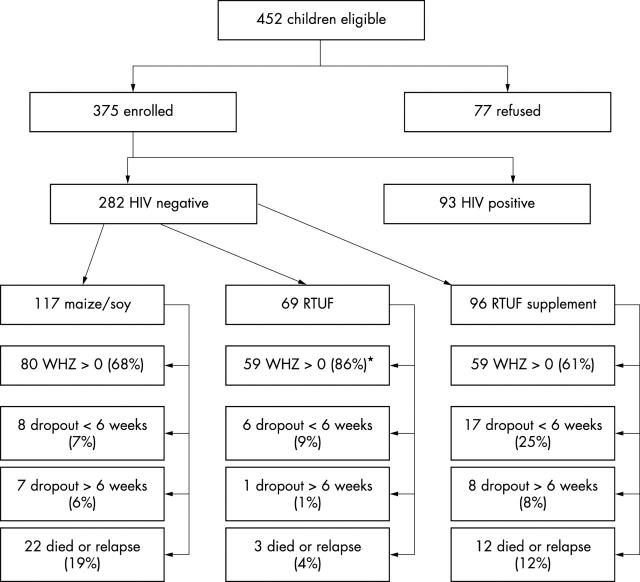
Methods: HIV negative children >1 year old discharged from the nutrition unit in Blantyre, Malawi were systematically allocated to one of three dietary regimens: RTUF, RTUF supplement, or blended maize/soy flour. RTUF and maize/soy flour provided 730 kJ/kg/day, while the RTUF supplement provided a fixed amount of energy, 2100 kJ/day. Children were followed fortnightly. Children completed the study when they reached WHZ >0, relapsed, or died. Outcomes were compared using a time-event model.
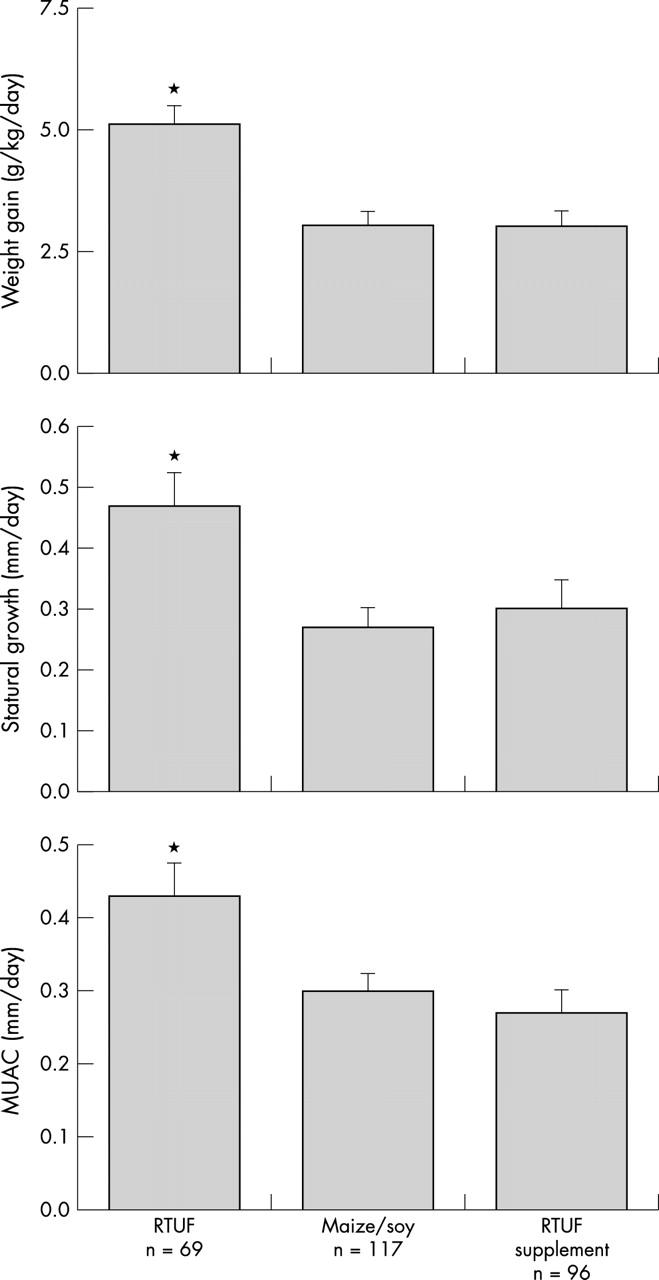
Results: A total of 282 children were enrolled. Children receiving RTUF were more likely to reach WHZ >0 than those receiving RTUF supplement or maize/soy flour (95% v 78%, RR 1.2, 95% CI 1.1 to 1.3). The average weight gain was 5.2 g/kg/day in the RTUF group compared to 3.1 g/kg/day for the maize/soy and RTUF supplement groups. Six months later, 96% of all children that reached WHZ >0 were not wasted.
Conclusions: Home based therapy of malnutrition with RTUF was successful; further operational work is needed to implement this promising therapy.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical