

Intraoperative subareolar radioisotope injection for immediate sentinel lymph node biopsy
- PMID: 15166963
- PMCID: PMC1356292
- DOI: 10.1097/01.sla.0000128304.13522.00
Intraoperative subareolar radioisotope injection for immediate sentinel lymph node biopsy
Abstract
Objective: To determine the identification of sentinel lymph node biopsy (SLNB) in breast cancer patients after intraoperative injection of unfiltered technetium-99m sulfur colloid (Tc-99) and blue dye.
Background: SLNB guided by a combination of radioisotope and blue dye injection yields the best identification rates in breast cancer patients. Radioisotope is given preoperatively, without local anesthesia, whereas blue dye is given intraoperatively. We hypothesized that, because of the rapid drainage noted with the subareolar injection technique of radioisotope, intraoperative injection would be feasible and less painful for SLN localization in breast cancer patients.
Methods: Intraoperative injection of Tc-99 and confirmation blue dye was performed using the subareolar technique for SLNB in patients with operable breast cancer. The time lapse between injection and axillary incision, the background count, the preincision and ex vivo counts of the hot nodes, and the axillary bed counts were documented. The identification rate was recorded.
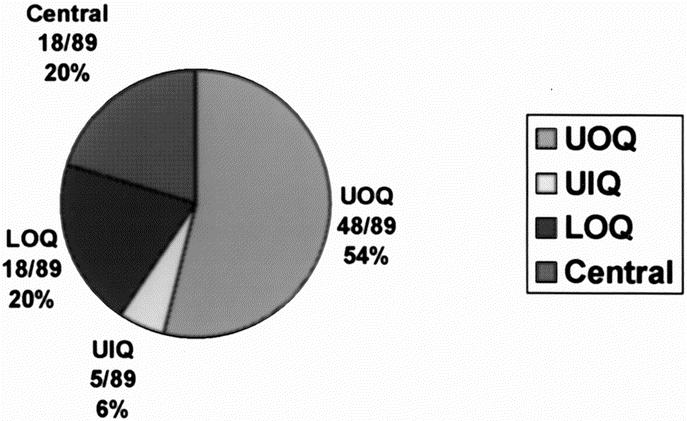
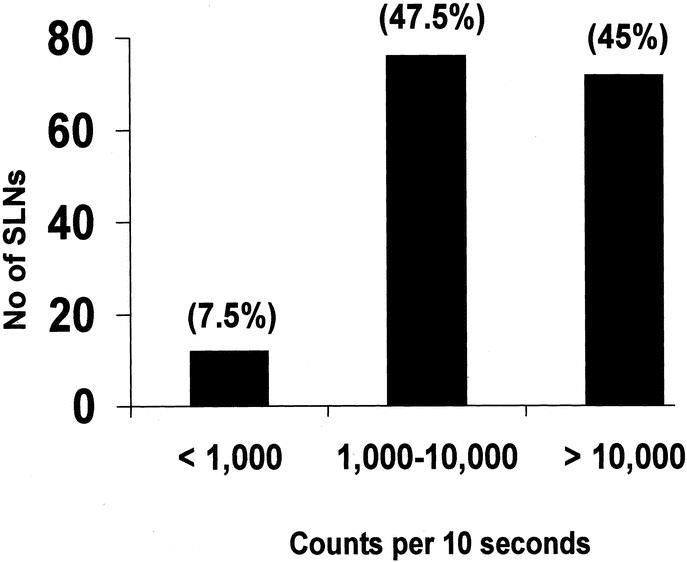
Results: Ninety-six SLNB procedures were done in 88 patients with breast cancer employing intraoperative subareolar injection technique for both radioisotope (all 96 procedures) and blue dye (93 procedures) injections. Ninety-three (97%) procedures had successful identification; all SLNs were hot; 91 (of 93 procedures with blue dye) were blue and hot. The mean time from radioisotope injection to incision was 19.9 minutes (SD 8.5 minutes). The mean highest 10 second count was 88,544 (SD 55,954). Three of 96 (3%) patients with failure of localization had previous excisional biopsies: 1 circumareolar and 2 upper outer quadrant incisions that may have disrupted the lymphatic flow.
Conclusion: Intraoperative subareolar injection of radioisotope rapidly drains to the SLNs and allows immediate staging of the axilla, avoiding the need to coordinate diagnostic services and a painful preoperative procedure.
Figures
References
-
- Schwartz GF, Guiliano AE, Veronesi U. Proceeding of the consensus conference of the role of sentinel lymph node biopsy in carcinoma or the breast April 19–22, 2001, Philadelphia, PA, USA [Review]. Breast J. 2002;8:124–138. - PubMed
-
- Albertini JJ, Lyman GH, Cox C, et al. Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA. 1996;276:1818–1822. - PubMed
-
- Pijpers R, Meijer S, Hoekstra OS, et al. Impact of lymphoscintigraphy on sentinel node identification with technetium-99-m-colloidal albumin in breast cancer. J Nucl Med. 1997;38:366–368. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
