

Symptom, family, and service predictors of children's psychiatric rehospitalization within one year of discharge
- PMID: 15187804
- PMCID: PMC2953818
- DOI: 10.1097/00004583-200404000-00010
Symptom, family, and service predictors of children's psychiatric rehospitalization within one year of discharge
Abstract
Objective: To investigate predictors of readmission to inpatient psychiatric treatment for children aged 5 to 12 discharged from acute-care hospitalization.
Method: One hundred nine children were followed for 1 year after discharge from inpatient care. Time to rehospitalization was the outcome of interest. Predictors of readmission, examined via the Cox proportional hazards model, were symptom and family factors assessed at admission, aspects of psychiatric treatment, and demographic variables.
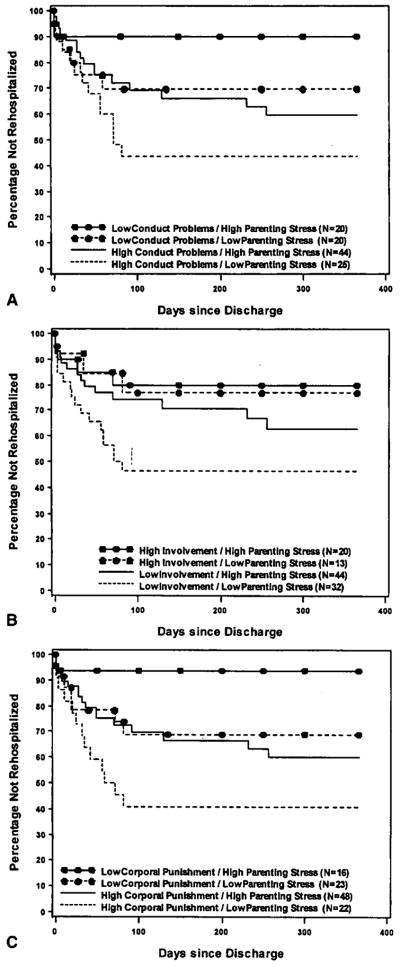
Results: The Kaplan-Meier rehospitalization risk within 1 year of discharge, taking into account known readmissions and censored observations, was 0.37. Most readmissions (81%) occurred within 90 days of discharge. Four variables contributed simultaneously to predicting readmission risk. More severe conduct problems, harsh parental discipline, and disengaged parent-child relations conferred a higher risk for rehospitalization; these risks were attenuated when parents disclosed higher stress in their parenting roles.
Conclusions: Findings showed that psychiatric rehospitalization of children is common, most likely in the trimester after discharge, and highly related to both child symptoms and family factors measurable at admission. Results suggest that efforts to improve postdischarge outcomes of children should target the initial period following inpatient care, address vigorously the complex treatment needs of those with severe conduct problems, and aim to improve parent-child relations.
Figures
References
-
- Abidin RR. Parenting Stress Index. 3. Odessa, FL: Psychological Assessment Resources; 1995.
-
- Achenbach TM. Integrative Guide for the 1991 CBCL/4–18, YSR and TRF Profiles. Burlington: University of Vermont Department of Psychiatry; 1991.
-
- Andersen R, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Memorial Fund Quarterly Health and Society. 1973;51:95–124. - PubMed
-
- Appleby L, Desai PN, Luchins DJ, Gibbons RD, Hedeker DR. Length of stay and recidivism in schizophrenia: a study of public psychiatric hospital patients. Am J Psychiatry. 1993;150:72–76. - PubMed
-
- Asarnow JR, Goldstein MJ, Carlson GA, Perdue S, Bates S, Keller J. Childhood-onset depressive disorders: a follow-up study of rates of rehospitalization and out-of-home placement among child psychiatric inpatients. J Affect Disord. 1988;15:245–253. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
