

A factorial trial of six interventions for the prevention of postoperative nausea and vomiting
- PMID: 15190136
- PMCID: PMC1307533
- DOI: 10.1056/NEJMoa032196
A factorial trial of six interventions for the prevention of postoperative nausea and vomiting
Abstract
Background: Untreated, one third of patients who undergo surgery will have postoperative nausea and vomiting. Although many trials have been conducted, the relative benefits of prophylactic antiemetic interventions given alone or in combination remain unknown.
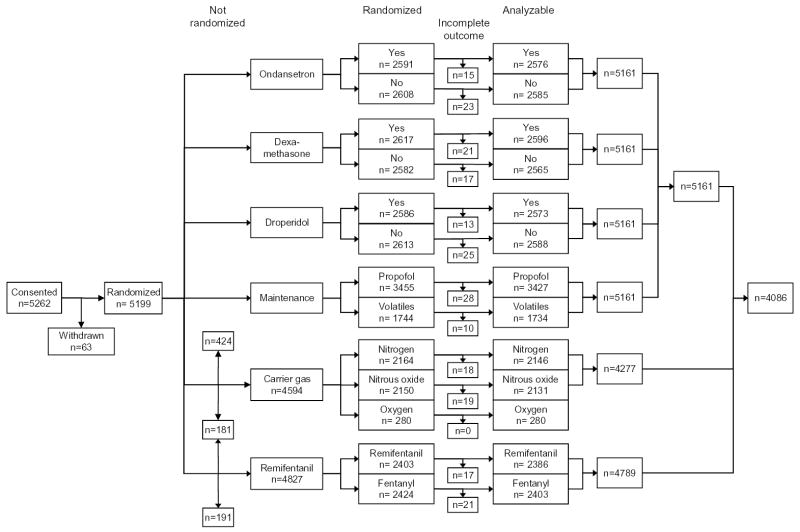
Methods: We enrolled 5199 patients at high risk for postoperative nausea and vomiting in a randomized, controlled trial of factorial design that was powered to evaluate interactions among as many as three antiemetic interventions. Of these patients, 4123 were randomly assigned to 1 of 64 possible combinations of six prophylactic interventions: 4 mg of ondansetron or no ondansetron; 4 mg of dexamethasone or no dexamethasone; 1.25 mg of droperidol or no droperidol; propofol or a volatile anesthetic; nitrogen or nitrous oxide; and remifentanil or fentanyl. The remaining patients were randomly assigned with respect to the first four interventions. The primary outcome was nausea and vomiting within 24 hours after surgery, which was evaluated blindly.
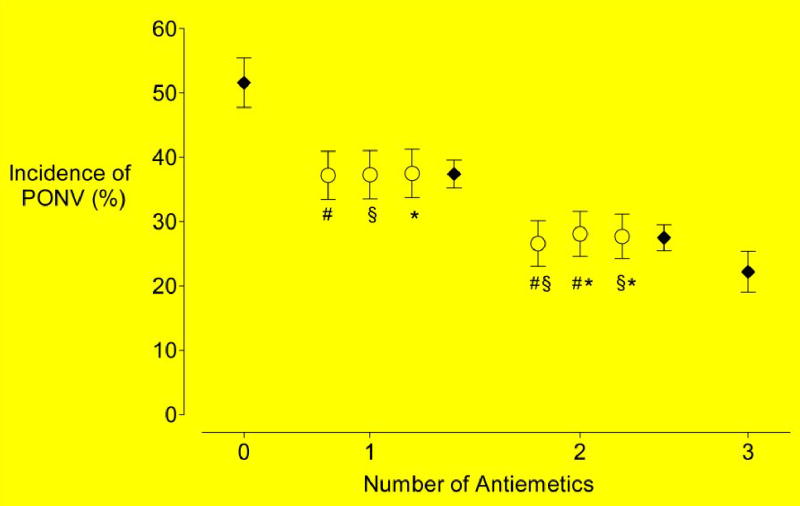
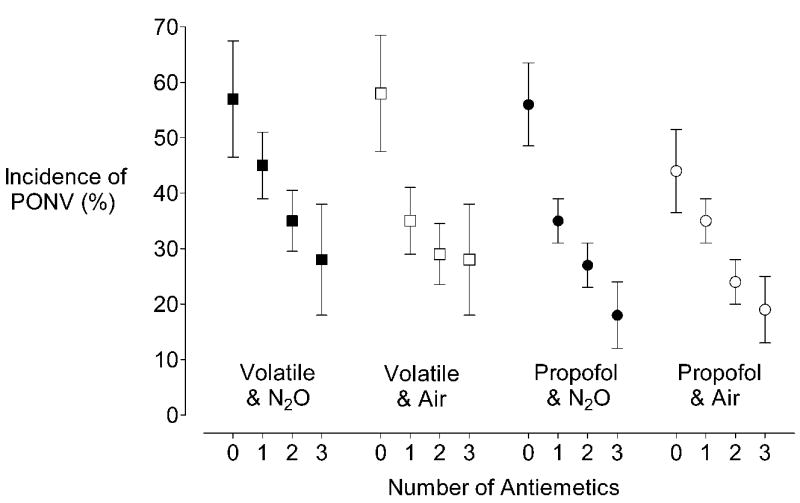
Results: Ondansetron, dexamethasone, and droperidol each reduced the risk of postoperative nausea and vomiting by about 26 percent. Propofol reduced the risk by 19 percent, and nitrogen by 12 percent; the risk reduction with both of these agents (i.e., total intravenous anesthesia) was thus similar to that observed with each of the antiemetics. All the interventions acted independently of one another and independently of the patients' baseline risk. Consequently, the relative risks associated with the combined interventions could be estimated by multiplying the relative risks associated with each intervention. Absolute risk reduction, though, was a critical function of patients' baseline risk.
Conclusions: Because antiemetic interventions are similarly effective and act independently, the safest or least expensive should be used first. Prophylaxis is rarely warranted in low-risk patients, moderate-risk patients may benefit from a single intervention, and multiple interventions should be reserved for high-risk patients.
Copyright 2004 Massachusetts Medical Society
Figures
Comment in
-
Prevention of postoperative nausea and vomiting--a multimodal solution to a persistent problem.N Engl J Med. 2004 Jun 10;350(24):2511-2. doi: 10.1056/NEJMe048099. N Engl J Med. 2004. PMID: 15190144 No abstract available.
-
Prevention of postoperative nausea and vomiting.N Engl J Med. 2004 Sep 30;351(14):1458-9; author reply 1458-9. doi: 10.1056/NEJM200409303511419. N Engl J Med. 2004. PMID: 15459310 No abstract available.
-
Prevention of postoperative nausea and vomiting.N Engl J Med. 2004 Sep 30;351(14):1458-9; author reply 1458-9. N Engl J Med. 2004. PMID: 15459994 No abstract available.
-
A factorial trial of six interventions for the prevention of postoperative nausea and vomiting.J Urol. 2005 Mar;173(3):887. doi: 10.1097/00005392-200503000-00072. J Urol. 2005. PMID: 15711308 No abstract available.
References
-
- Gan TJ. Postoperative nausea and vomiting--can it be eliminated? JAMA. 2002;287:1233–6. - PubMed
-
- Kovac AL. Prevention and treatment of postoperative nausea and vomiting. Drugs. 2000;59:213–243. - PubMed
-
- Watcha MF. Postoperative nausea and emesis. Anesthesiol Clin North America. 2002;20:471–84. - PubMed
-
- Koivuranta M, Laara E, Snare L, Alahuhta S. A survey of postoperative nausea and vomiting. Anaesthesia. 1997;52:443–449. - PubMed
-
- Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients Anesth Analg. 1999;89:652–658. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical