

Executive processes in Parkinson's disease: FDG-PET and network analysis
- PMID: 15195290
- PMCID: PMC6871801
- DOI: 10.1002/hbm.20033
Executive processes in Parkinson's disease: FDG-PET and network analysis
Abstract
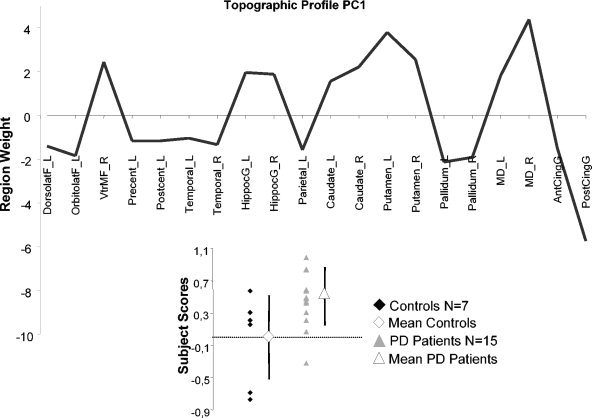
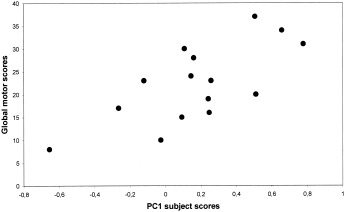
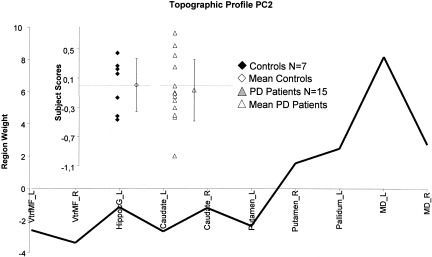
It is assumed widely that the clinical expression of Parkinson's Disease (PD), both motor and cognitive, is subtended by topographically distributed brain networks. However, little is known about the functional neuroanatomy of executive dysfunction in PD. Our objective was to validate further in a PD group the use of network analysis to assess the relationship between executive processes and pathological disorganization of frontostriatal networks. We studied 15 patients with idiopathic PD, and 7 age-matched normal controls, using resting [(18)F]fluorodeoxyglucose (FDG) and high-resolution positron emission tomography (PET). We carried out network analysis on regional metabolic data to identify specific covariation patterns associated with motor and executive dysfunction. We detected two independent patterns relating respectively to the two clinical abnormalities. The first pattern (principal component 1) was topographically similar to that described previously in other PD populations. Subject scores for this pattern discriminated patients from controls and correlated significantly with bradykinesia ratings (P = 0.013, r = 0.655) in PD patients. The second pattern (principal component 2) was characterized by relative ventromedial frontal, hippocampal, and striatal hypometabolism, associated with mediodorsal thalamic hypermetabolism. In the PD group, scores from this pattern correlated with scores on the conditional associative learning (CAL; P = 0.01, r = 0.690) and the Brown Peterson paradigm (BPP; P = 0.017, r = -0.651) tests, respectively assessing strategy and planning, and working memory. According to these findings, the networks subserving bradykinesia and executive dysfunction in PD seems to be topographically distinct and to involve different aspects of subcortico-cortical processing.
Copyright 2004 Wiley-Liss, Inc.
Figures

References
-
- Alexander GE, Crutcher MD, DeLong MR (1990): Basal ganglia‐thalamocortical circuits: parallel substrates for motor, oculomotor, “prefrontal” and “limbic” functions. Prog Brain Res 85: 119–146. - PubMed
-
- Allain P, Travere JM, Baron JC, Bloyet D (1992): Multimodal analysis of brain images by superimposition of information from PET, 3‐D‐RMI and atlas data bases. Acta Stereologica, Proceedings of the Eighth International Congress for Stereology. 11: 181–185.
-
- Baddeley A (2000): The episodic buffer: a new component of working memory? Trends Cogn Sci 4: 417–423. - PubMed
-
- Bernheimer H, Birkmayer W, Hornykiewicz O, Jellinger K, Seitelberger F (1973): Brain dopamine and the syndromes of Parkinson and Huntington. Clinical, morphological and neurochemical correlations. J Neurol Sci 20: 415–455. - PubMed
-
- Brück A, Portin R, Lindell A, Laihinen A, Bergman J, Haaparanta M, Solin O, Rinne JO (2001): Positron emission tomography shows that impaired frontal lobe functioning in Parkinson's disease is related to dopaminergic hypofunction in the caudate nucleus. Neurosci Lett 311: 81–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
