

Long term risk stratification of patients with acute coronary syndromes: characteristics of troponin T testing and continuous ST segment monitoring
- PMID: 15201240
- PMCID: PMC1768301
- DOI: 10.1136/hrt.2003.020479
Long term risk stratification of patients with acute coronary syndromes: characteristics of troponin T testing and continuous ST segment monitoring
Abstract
Objective: To examine the long term prognostic characteristics of troponin T testing and continuous multi-lead ST segment monitoring in combination with clinical and 12 lead ECG risk indicators in patients with acute coronary syndromes (ACS).
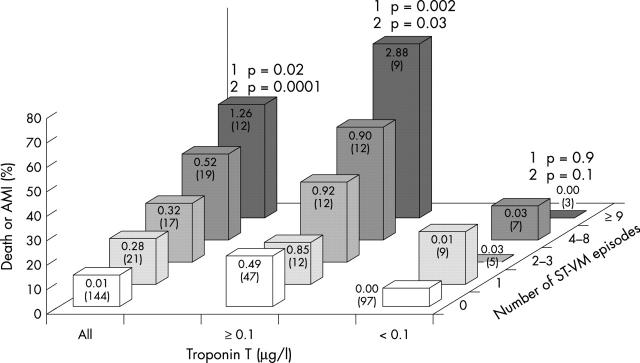
Patients and design: Patients with suspected ACS (n = 213) were studied. Troponin T was analysed in blood samples collected during the first 12 hours after admission. Continuous vectorcardiography ST segment monitoring was performed for 24 hours and the number of ST vector magnitude episodes was registered. Patients were followed up for a median of 28 months. The end point was a composite of cardiac death and acute myocardial infarction.
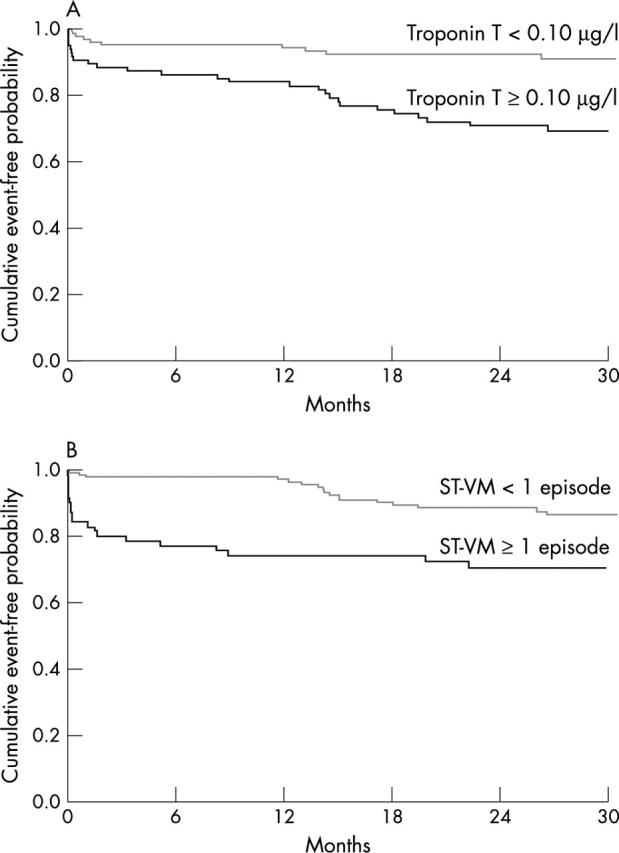
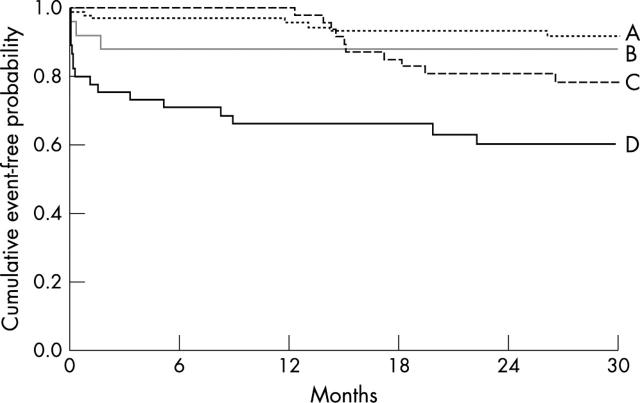
Results: Thirty eight (18%) patients reached the composite end point. The median (interquartile range) time from study inclusion to the time of the composite end point was longer for patients predicted to be at risk by troponin T testing (n = 27) than for those predicted to be at risk by ST segment monitoring (n = 20) (8.4 (0.2-15) months v 0.3 (0.1-4.3) months, p = 0.04). Significant univariate predictors of the composite end point were age > or = 65 years, diabetes, previous myocardial infarction, congestive heart failure, use of beta blockers or diuretics at admission, 12 lead ECG ST segment depression at admission, troponin T concentration > or = 0.10 microg/l, and > or = 1 ST vector magnitude episodes. Age > or = 65 years, previous myocardial infarction, and troponin T concentration > or = 0.10 microg/l provided independent prognostic information after multivariate analysis of potential risk variables. The prognostic value of transient ischaemic episodes in ACS seems to be confined to the short term.
Conclusions: Both biochemical and continuous ECG markers reflect an increased risk for patients with ACS; however, the methods exhibit different temporal risk characteristics.
Figures
Comment in
-
Risk stratification in acute coronary syndrome: focus on unstable angina/non-ST segment elevation myocardial infarction.Heart. 2004 Jul;90(7):729-31. doi: 10.1136/hrt.2004.034546. Heart. 2004. PMID: 15201236 Free PMC article.
Similar articles
-
Combined prognostic utility of ST segment in lead aVR and troponin T on admission in non-ST-segment elevation acute coronary syndromes.Am J Cardiol. 2006 Feb 1;97(3):334-9. doi: 10.1016/j.amjcard.2005.08.049. Am J Cardiol. 2006. PMID: 16442391
-
The combination of a continuous 12-lead ECG and troponin T; a valuable tool for risk stratification during the first 6 hours in patients with chest pain and a non-diagnostic ECG.Eur Heart J. 2000 Sep;21(17):1464-72. doi: 10.1053/euhj.2000.2178. Eur Heart J. 2000. PMID: 10952839
-
Independent prognostic value of serum creatine kinase isoenzyme MB mass, cardiac troponin T and myosin light chain levels in suspected acute myocardial infarction. Analysis of 28 months of follow-up in 196 patients.J Am Coll Cardiol. 1995 Mar 1;25(3):574-81. doi: 10.1016/0735-1097(94)00430-X. J Am Coll Cardiol. 1995. PMID: 7860899
-
Strategies for clinical assessment of patients with suspected acute coronary syndromes.Scand J Clin Lab Invest Suppl. 1999;230:36-42. Scand J Clin Lab Invest Suppl. 1999. PMID: 10389200 Review.
-
Troponin: an important prognostic marker and risk-stratification tool in non-ST-segment elevation acute coronary syndromes.J Am Coll Cardiol. 2003 Feb 19;41(4 Suppl S):31S-36S. doi: 10.1016/s0735-1097(02)02832-2. J Am Coll Cardiol. 2003. PMID: 12644338 Review.
Cited by
-
Risk stratification in acute coronary syndrome: focus on unstable angina/non-ST segment elevation myocardial infarction.Heart. 2004 Jul;90(7):729-31. doi: 10.1136/hrt.2004.034546. Heart. 2004. PMID: 15201236 Free PMC article.
References
-
- Wu AHB, Abbas SA, Green S, et al. Prognostic value of cardiac troponin T in unstable angina pectoris. Am J Cardiol 1995;76:970–2. - PubMed
-
- Ravkilde J , Nissen H, Hørder M, et al. Independent prognostic value of serum creatine kinase isoenzyme MB mass, cardiac troponin T and myosin light chain levels in suspected acute myocardial infarction. Analysis of 28 months follow-up in 196 patients. J Am Coll Cardiol 1995;25:574–81. - PubMed
-
- Ohman EM, Armstrong PW, Christenson RH, et al. Cardiac troponin T levels for risk stratification in acute myocardial ischemia. N Engl J Med 1996;335:1333–41. - PubMed
-
- Stubbs P , Collinson P, Mosely D, et al. Prognostic significance of admission troponin T concentrations in patients with myocardial infarction. Circulation 1996;94:1291–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical