

Cerebellar vermian atrophy after neonatal hypoxic-ischemic encephalopathy
- PMID: 15205139
- PMCID: PMC7975683
Cerebellar vermian atrophy after neonatal hypoxic-ischemic encephalopathy
Abstract
Background and purpose: Although pathologic evidence of cerebellar injury due to birth asphyxia is well described, neuroimaging evidence is sparse. The primary purpose of this retrospective study was to evaluate the early and late imaging findings in the cerebellum of patients who had neonatal hypoxic-ischemic encephalopathy with thalamic edema shown by neonatal CT. The secondary aims were to validate thalamic edema shown by neonatal CT as a marker of thalamic injury and to assess the late cerebral cortical abnormalities associated with neonatal thalamic edema.
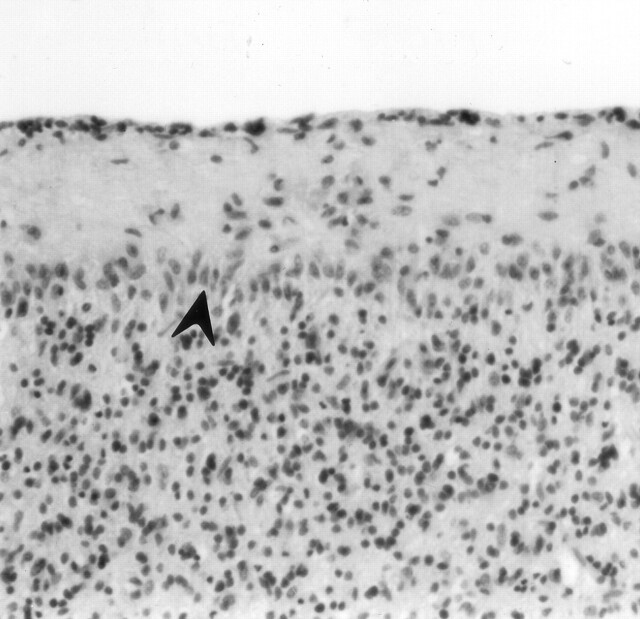
Methods: Fifty-five neonates with thalamic edema shown by CT performed when patients were 3 days old were identified from a cohort of full-term neonates with hypoxic-ischemic encephalopathy. Twenty-six of the 55 underwent follow-up neuroimaging. All sonograms, CT scans, and MR images of the brains of the 55 neonates were retrospectively reviewed by two pediatric neuroradiologists. The examinations were reviewed for evidence of hemorrhage, edema, atrophy, and CT attenuation or MR signal intensity abnormalities in the cerebellum, basal ganglia, and cerebral cortex. The neonatal autopsy findings in four cases were reviewed separately by a pediatric neuropathologist.
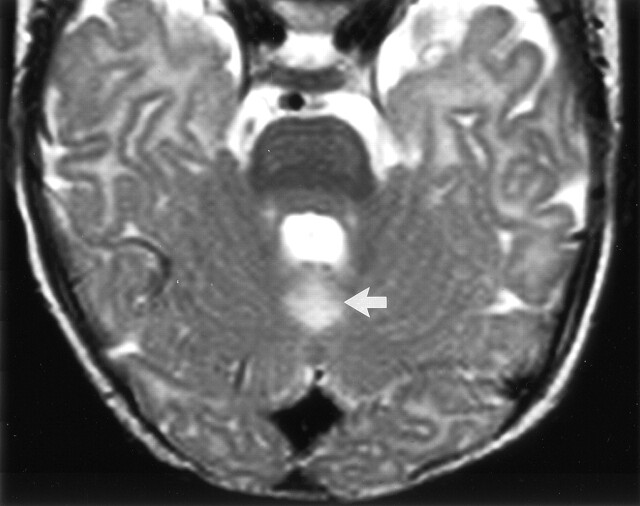
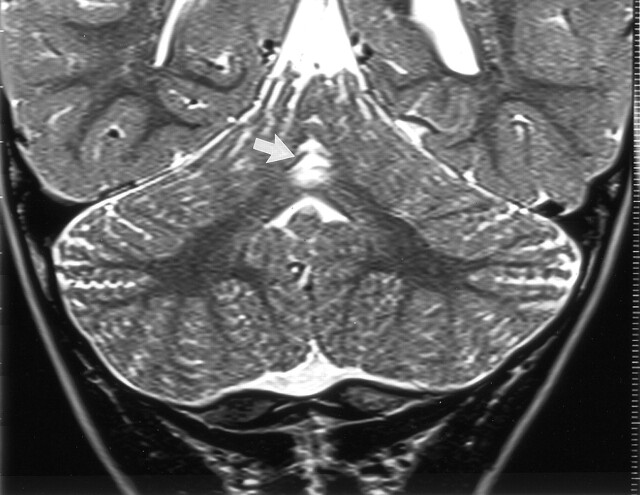
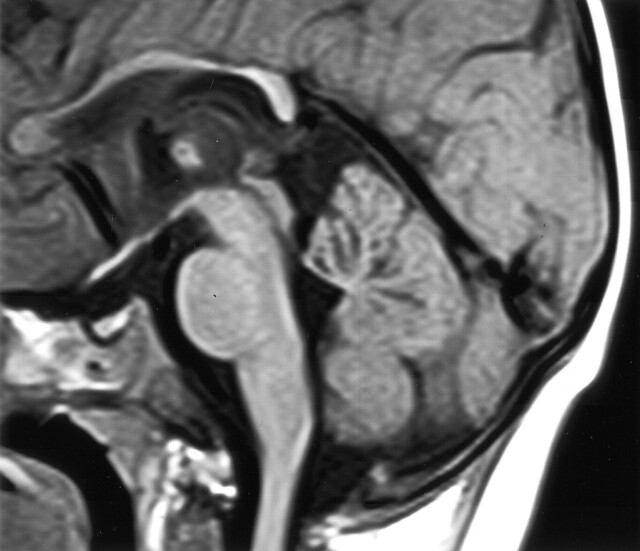
Results: Of the 55 neonates with thalamic edema shown by neonatal CT, 28 (51%) had thalamic edema with diffuse cerebral cortical edema, and 27 (49%) had thalamic edema without diffuse cortical edema. The cerebellar vermes appeared normal on all neonatal sonograms, CT scans, and MR images. However, atrophy of the cerebellar vermis was found in 12 (46%) of 26 patients by use of follow-up studies (95% CI, 27-65%). One of the 12 patients also had cerebellar hemispheric atrophy. Cerebellar vermian atrophy was shown at follow-up in eight (67%) of 12 patients who had neonatal thalamic edema with cortical sparing, compared with four (29%) of 14 patients who had thalamic edema with diffuse cortical edema. The difference did not reach statistical significance. The thalami appeared abnormal on follow-up neuroimages in 25 of 26 cases. Different patterns of cortical atrophy were observed on the images of patients who had thalamic edema with cortical sparing compared with those obtained in patients who had thalamic edema with cortical involvement.
Conclusion: Cerebellar vermian atrophy is a frequent finding on follow-up images of patients in whom neonatal CT showed hypoxic-ischemic encephalopathy with abnormal thalami.
Figures


References
-
- Chugani HT, Phelps ME. Maturational changes in cerebral function in infants determined by 18 FDG positron emission tomography. Science 1986;231:840–843 - PubMed
-
- Ashwal S, Majcher JS, Vain N, Longo LD. Patterns of fetal lamb regional cerebral blood flow during and after prolonged hypoxia. Pediatr Res 1980;14:1104–1110 - PubMed
-
- Pasternak JF, Gorey MT. The syndrome of acute near-total intrauterine asphyxia in the term infant. Pediatr Neurol 1998;18:391–398 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources