

Case Reports
MR imaging of brain-stem hypoplasia in horizontal gaze palsy with progressive scoliosis
Affiliations
- PMID: 15205146
- PMCID: PMC7975651
Item in Clipboard
Case Reports
MR imaging of brain-stem hypoplasia in horizontal gaze palsy with progressive scoliosis
AJNR Am J Neuroradiol.
2004 Jun-Jul.
Abstract
We present the MR imaging findings of a girl with horizontal gaze palsy and progressive scoliosis (HGPPS). HGPPS is a rare congenital disorder characterized by absence of conjugate horizontal eye movements and accompanied by progressive scoliosis developing in childhood and adolescence. MR imaging depicted brain-stem hypoplasia with absence of the facial colliculi, presence of a deep midline pontine cleft (split pons sign), and a butterfly configuration of the medulla. These MR imaging features suggest the diagnosis of HGPPS and correlate with the clinical findings. We hypothesize that maldevelopment of dorsomedial brain-stem structures plays a crucial role in the pathogenesis of HGPPS.
Figures
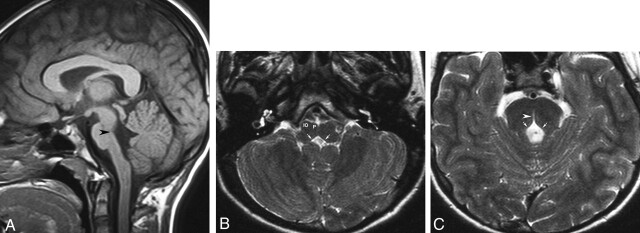
MR images obtained in a 13-year-old girl with early-onset thoracolumbar scoliosis. A, Sagittal T1-weighted image (500/12 [TR/TE]) of the brain shows depression of the floor of the fourth ventricle (arrowhead). The pons and medulla oblongata have a reduced volume. B, Axial T2-weighted image (4500/120) at the level of the medulla oblongata shows rectangular configuration of the medulla. The floor of the fourth ventricle is tent shaped (arrows), with missing prominence of the cuneate and gracile nuclei. The inferior olivary nuclei (IO) are prominent with respect to the pyramids (P). C, Axial T2-weighted image (4500/120) at the level of the pons shows absence of the facial colliculi, with tent-shaped configuration of the floor of the fourth ventricle (arrows). A deep midsagittal cleft extends ventrally from the fourth ventricular floor, producing the split pons sign (arrowhead).
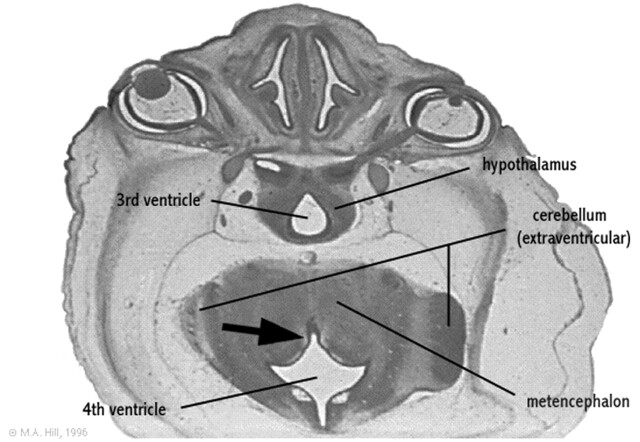
Rendering of the embryologic development of the fourth ventricle. Axial section of a 27-mm human embryo (approximately day 56 and Carnegie stage 22) shows ventral fourth ventricular furrow (arrow) deeply indenting the posterior aspect of the developing metencephalon. Modified from M. Hill, UNSW Embryology, version 3.0 (8), with permission.
References
-
- Crisfield RJ. Scoliosis with progressive external ophthalmoplegia in four siblings. J Bone Joint Surg 1974;56B:484–489 - PubMed
-
- Dretakis EK, Kondoyannis PN. Congenital scoliosis associated with encephalopathy in five children of two families. J Bone Joint Surg 1974;56A:1747–1750 - PubMed
-
- Sharpe JA, Silversides JL, Blair RD. Familial paralysis of horizontal gaze: associated with pendular nystagmus, progressive scoliosis, and facial contraction with myokymia. Neurology 1975;25:1035–1040 - PubMed
-
- Thomsen M, Steffen H, Sabo D, Niethard FU. Juvenile progressive scoliosis and congenital horizontal gaze palsy. J Pediatr Orthop B 1996;5:185–189 - PubMed
-
- Jen J, Coulin CJ, Bosley TM, et al. Familial horizontal gaze palsy with progressive scoliosis maps to chromosome 11q23–25. Neurology 2002;59:432–435 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical