

Intra-arterial nimodipine for the treatment of symptomatic cerebral vasospasm after aneurysmal subarachnoid hemorrhage: preliminary results
- PMID: 15205150
- PMCID: PMC7975655
Intra-arterial nimodipine for the treatment of symptomatic cerebral vasospasm after aneurysmal subarachnoid hemorrhage: preliminary results
Abstract
Background and purpose: Cerebral vasospasm remains a major problem in patients recovering from aneurysmal subarachnoid hemorrhage despite advances in medical, surgical, and endovascular care. Our purpose was to assess the efficacy of intra-arterial nimodipine, a calcium-channel blocker acting mainly on cerebral vessels, in preventing delayed neurologic deficits in patients with symptomatic vasospasm.
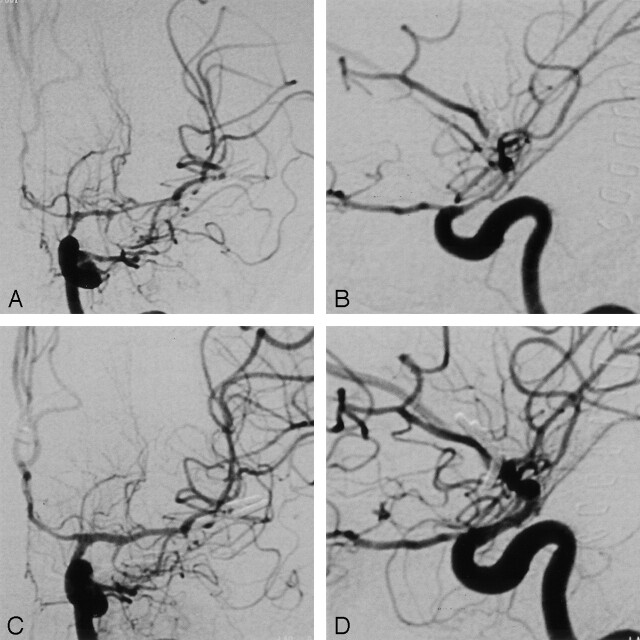
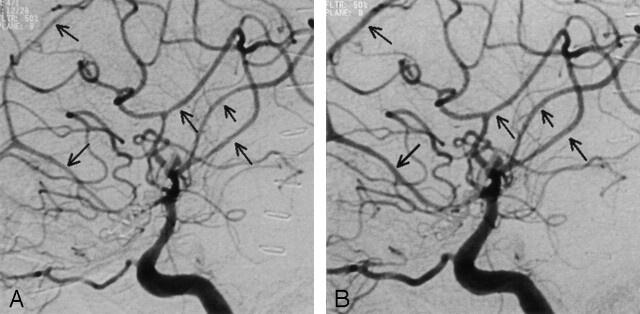
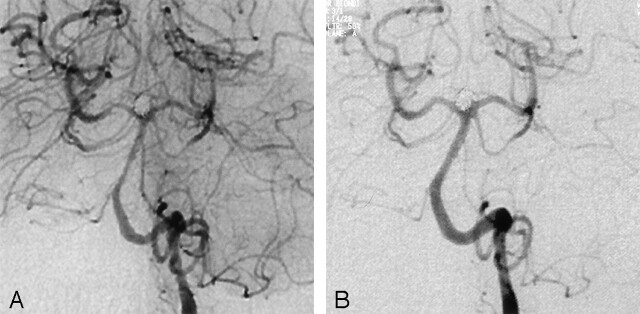
Methods: Clinical charts of 25 consecutively treated patients were retrospectively reviewed. A multifactorial decision tree was used to determine the indication for angiography and subsequent endovascular treatment. Nimodipine was infused intra-arterially via a diagnostic catheter in the internal carotid artery or vertebral artery at a rate of 0.1 mg/min. Angiographic vasospasm before endovascular treatment, immediate vessel caliber modifications, and short- and long-term clinical efficacy of the procedure were assessed.
Results: Thirty procedures were performed in 25 patients. Clinical improvement was observed in 19 (76%), 16 of whom improved after the first endovascular procedure, two after the second intra-arterial treatment, and one after the third. Of these 19 patients, only 12 (63%) had notable vascular dilatation at postprocedural angiography. Dilatation of infused vessels occurred in only 13 (43%) of 30 procedures. After follow-up of 3-6 months, 18 (72%) of 25 patients had a favorable outcome (Glasgow outcome scale score of 1-2 and modified Rankin scale score of 0-2). No complications were observed.
Conclusion: Intra-arterial nimodipine is effective and safe for the treatment of symptomatic vasospasm after subarachnoid hemorrhage. Further prospective randomized studies of cerebral blood flow are needed to confirm these results.
Figures
References
-
- Weir B, MacDonald L. Cerebral vasospasm. Clin Neurosurg 1993;40:40–55 - PubMed
-
- Paoletti C, Dematons C, Bellec C, et al. Medical management of vasospasm and hemodynamic alterations in the neurosurgical ICU. In: Connors JI, Wojak J, eds. Interventional Neuroradiology: Strategies and Practical Techniques. Philadelphia: WB Saunders Company;2000;602–612
-
- Song JK, Elliott JP, Eskridge JM. Neuroradiologic diagnosis and treatment of vasospasm. Neuroimaging Clin N Am 1997;7:819–835 - PubMed
-
- Rosenwasser RH, Armonda RA, Thomas JE, Benitez RP, Gannon PM, Harrop J Therapeutic modalities for the management of cerebral vasospasm: timing of endovascular options. Neurosurgery 1999;44:975–979; discussion 979–980 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources