

Effects of hydrofluoroalkane formulations of ciclesonide 400 microg once daily vs fluticasone 250 microg twice daily on methacholine hyper-responsiveness in mild-to-moderate persistent asthma
- PMID: 15206989
- PMCID: PMC1884548
- DOI: 10.1111/j.1365-2125.2004.02108.x
Effects of hydrofluoroalkane formulations of ciclesonide 400 microg once daily vs fluticasone 250 microg twice daily on methacholine hyper-responsiveness in mild-to-moderate persistent asthma
Abstract
Aims: There are no data comparing the relative efficacy of hydrofluoroalkane (HFA) formulations of ciclesonide (CIC) and fluticasone propionate (FP) on airway hyper-responsiveness, in mild-to-moderate persistent asthma. We therefore elected to evaluate the comparative efficacy of HFA pressurized metered-dose inhaler formulations of CIC and FP, assessing methacholine challenge, in addition to exhaled nitric oxide, lung function, diary cards and quality of life.
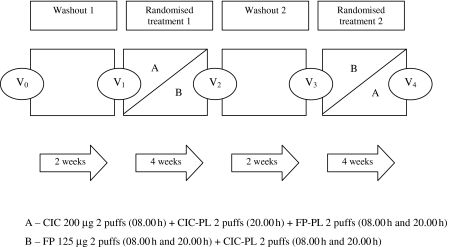
Methods: Nineteen mild-to-moderate asthmatic patients completed the study per protocol in randomized, double-blind, double-dummy, crossover fashion. Patients were required to stop their usual inhaled corticosteroid therapy for the duration of the study. Patients were commenced instead on salmeterol (SM) 50 microg one puff twice daily + montelukast (ML) 10 mg once daily for 2-week washout periods prior to each randomized treatment, in order to prevent dropouts. Patients received 4 weeks of either CIC 200 microg two puffs once daily (08.00 h) + CIC-placebo (PL) two puffs once daily (20.00 h) + FP-PL two puffs twice daily (08.00 h and 20.00 h), or FP 125 microg two puffs twice daily (08.00 h and 20.00 h) + CIC-PL two puffs twice daily (08.00 h and 20.00 h). SM + ML were withheld for 72 h prior to post-washout visits and CIC or FP was withheld for 24 h prior to study visits.
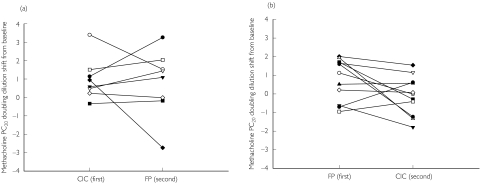
Results: There was no significant difference between CIC vs. FP for the primary outcome of methacholine PC20 as doubling dilution (dd) shift from respective baseline; mean difference: 0.4 dd (95% CI -0.4, 1.2). Moreover, there was no difference between treatments for the sequence of CIC first vs FP second; mean difference: 0.2 dd (95% CI -1.3, 1.7) or FP first vs CIC second; mean difference: 0.9 dd (95% CI -0.1, 1.8). There were also no differences for other secondary outcomes between treatments, either respective or irrespective of sequence, as change from baseline.
Conclusions: There were no differences between 4 weeks of CIC 400 microg once daily and FP 250 microg twice daily on methacholine hyper-responsiveness in mild-to-moderate persistent asthma. Longer-term studies are indicated to evaluate their relative efficacy on asthma exacerbations.
Figures
References
-
- National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma Update on Selected Topics – 2002. J Allergy Clin Immunol. 2002;110:S141–S219. - PubMed
-
- Wilson AM, Lipworth BJ. Dose–response evaluation of the therapeutic index for inhaled budesonide in patients with mild-to-moderate asthma. Am J Med. 2000;108:269–75. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
