

What can family physicians offer patients with carpal tunnel syndrome other than surgery? A systematic review of nonsurgical management
- PMID: 15209206
- PMCID: PMC1466671
- DOI: 10.1370/afm.21
What can family physicians offer patients with carpal tunnel syndrome other than surgery? A systematic review of nonsurgical management
Abstract
Background: We undertook a literature review to produce evidence-based recommendations for nonsurgical family physician management of carpal tunnel syndrome (CTS).
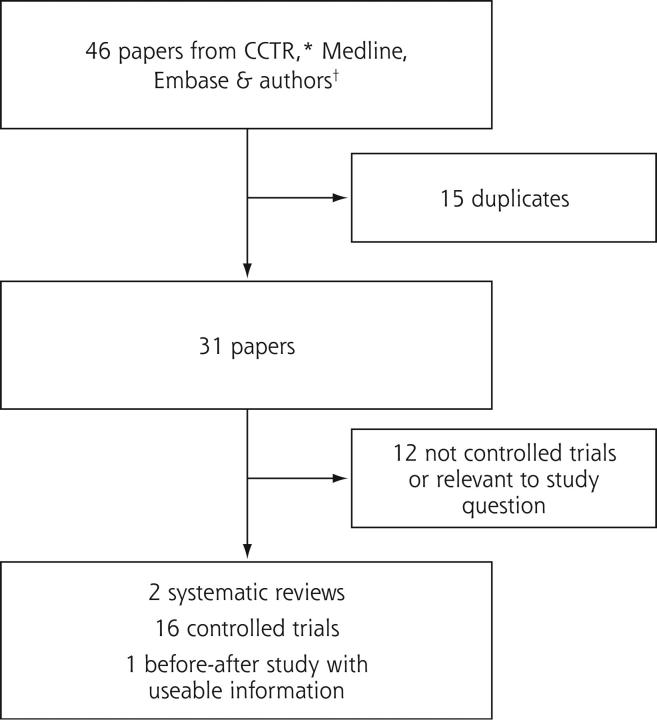
Methods: Study design was systematic review of randomized controlled trials (RCTs) on CTS treatment. Data sources were English publications from all relevant databases, hand searches, and guidelines. Outcomes measured were nonsurgical management options for CTS.
Results: We assessed 2 systematic reviews, 16 RCTs, and 1 before-and-after study using historical controls. A considerable percentage of CTS resolves spontaneously. There is strong evidence that local corticosteroid injections, and to a lesser extent oral corticosteroids, give short-term relief for CTS sufferers. There is limited evidence to indicate that splinting, laser-acupuncture, yoga, and therapeutic ultrasound may be effective in the short to medium term (up to 6 months). The evidence for nerve and tendon gliding exercises is even more tentative. The evidence does not support the use of nonsteroidal anti-inflammatory drugs, diuretics, pyridoxine (vitamin B6), chiropractic treatment, or magnet treatment.
Conclusions: For those who are not able to get surgery or for those who do not want surgery, there are some conservative modalities that can be tried. These modalities include ones for which there is good evidence. It would be reasonable to try some of the techniques with less evidence if the better ones are not successful. Reconsideration of surgery must always be kept in mind to avoid permanent nerve damage.
Similar articles
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.Health Technol Assess. 2006 Nov;10(46):1-233, i-iv. doi: 10.3310/hta10460. Health Technol Assess. 2006. PMID: 17083854
-
Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome.Cochrane Database Syst Rev. 2003;2003(1):CD003219. doi: 10.1002/14651858.CD003219. Cochrane Database Syst Rev. 2003. PMID: 12535461 Free PMC article.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.Health Technol Assess. 2006 Sep;10(34):iii-iv, ix-xi, 1-204. doi: 10.3310/hta10340. Health Technol Assess. 2006. PMID: 16959170
-
Interventions for promoting habitual exercise in people living with and beyond cancer.Cochrane Database Syst Rev. 2018 Sep 19;9(9):CD010192. doi: 10.1002/14651858.CD010192.pub3. Cochrane Database Syst Rev. 2018. PMID: 30229557 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
Cited by
-
Therapeutic ultrasound for carpal tunnel syndrome.Cochrane Database Syst Rev. 2013 Mar 28;2013(3):CD009601. doi: 10.1002/14651858.CD009601.pub2. Cochrane Database Syst Rev. 2013. PMID: 23543580 Free PMC article.
-
A comparison of the lidocaine patch 5% vs naproxen 500 mg twice daily for the relief of pain associated with carpal tunnel syndrome: a 6-week, randomized, parallel-group study.MedGenMed. 2006 Aug 9;8(3):33. MedGenMed. 2006. PMID: 17406167 Free PMC article. Clinical Trial.
-
Quality analysis of prior systematic reviews of carpal tunnel syndrome: an overview of the literature.Sao Paulo Med J. 2022 Dec 19;141(5):e20211020. doi: 10.1590/1516-3180.2021.1020.R2.10102022. eCollection 2022. Sao Paulo Med J. 2022. PMID: 36541951 Free PMC article.
-
In vitro optimization of dexamethasone phosphate delivery by iontophoresis.Phys Ther. 2008 Oct;88(10):1177-85. doi: 10.2522/ptj.20080043. Epub 2008 Aug 21. Phys Ther. 2008. PMID: 18719003 Free PMC article.
-
Comparison of Two Manual Therapy Programs, including Tendon Gliding Exercises as a Common Adjunct, While Managing the Participants with Chronic Carpal Tunnel Syndrome.Pain Res Manag. 2022 Jun 8;2022:1975803. doi: 10.1155/2022/1975803. eCollection 2022. Pain Res Manag. 2022. PMID: 35719196 Free PMC article. Clinical Trial.
References
-
- Practice parameter for carpal tunnel syndrome [summary statement]. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 1993;43:2406–2409. - PubMed
-
- Stevens JC, Sun S, Beard CM, O’Fallon WM, Kurland LT. Carpal tunnel syndrome in Rochester, Minnesota, 1961 to 1980. Neurology. 1988;38:134–138. - PubMed
-
- Marshall S. Carpal tunnel syndrome. Clin Evid. 2001;5:717–728.
-
- Spinner RJ, Bachman JW, Amadio PC. The many faces of carpal tunnel syndrome. Mayo Clin Proc. 1989;64:829–836. - PubMed
-
- Mackinnon SE, Novak CB. Repetitive strain in the workplace. J Hand Surg [Am]. 1997;22:2–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials