

Suboptimal statin adherence and discontinuation in primary and secondary prevention populations
- PMID: 15209602
- PMCID: PMC1492382
- DOI: 10.1111/j.1525-1497.2004.30516.x
Suboptimal statin adherence and discontinuation in primary and secondary prevention populations
Abstract
Objectives: To compare statin nonadherence and discontinuation rates of primary and secondary prevention populations and to identify factors that may affect those suboptimal medication-taking behaviors.
Design: Retrospective cohort utilizing pharmacy claims and administrative databases.
Setting: A midwestern U.S. university-affiliated hospital and managed care organization (MCO).
Patients: Non-Medicaid MCO enrollees, 18 years old and older, who filled 2 or more statin prescriptions from January 1998 to November 2001; 2258 secondary and 2544 primary prevention patients were identified.
Measurements: Nonadherence was assessed by the percent of days without medication (gap) over days of active statin use, a measurement known as cumulative multiple refill-interval gap (CMG). Discontinuation was identified by cessation of statin refills prior to the end of available pharmacy claims data.
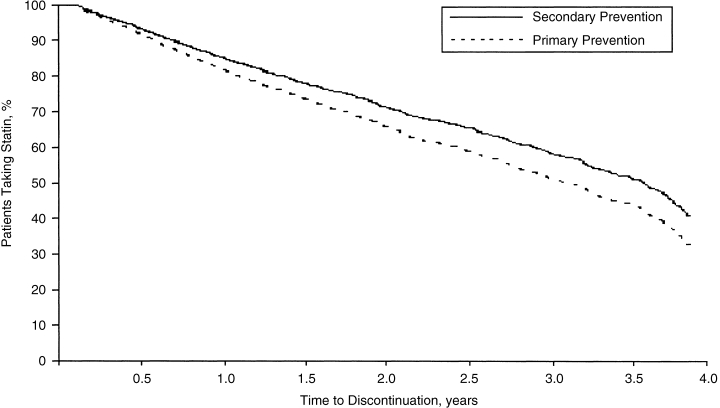
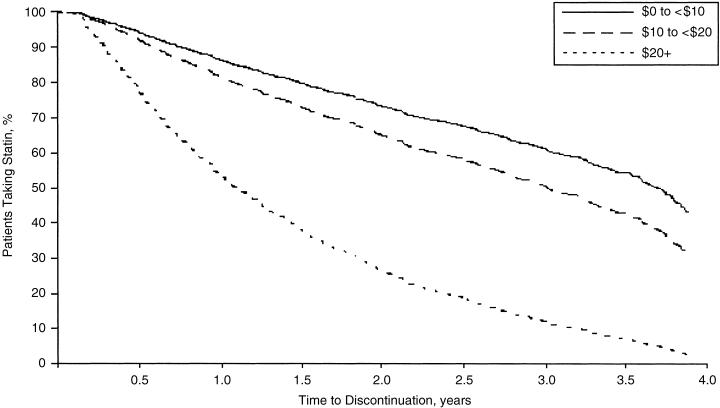
Results: On average, the primary and secondary groups went without medication 20.4% and 21.5% of the time, respectively (P=.149). Primary prevention patients were more likely to discontinue statin therapy relative to the secondary prevention cohort (relative risk [RR], 1.24; 95% confidence interval [CI], 1.08 to 1.43). Several factors influenced nonadherence and discontinuation. Fifty percent of patients whose average monthly statin copayment was < US dollars 10 discontinued by the end of follow-up (3.9 years), whereas 50% of those who paid >US dollars 10 but <or=US dollars 20 and >US dollars 20 discontinued by 2.2 and 1.0 years, respectively (RR, 1.39 and 4.30 relative to <US dollars 10 copay, respectively).
Conclusions: Statin nonadherence and discontinuation was suboptimal and similar across prevention categories. Incremental efforts, including those that decrease out-of-pocket pharmaceutical expenditures, should focus on improving adherence in high-risk populations most likely to benefit from statin use.
Figures
References
-
- Shepherd J, Cobe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia: West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301–7. - PubMed
-
- Bradford RH, Shear CL, Chremos AN, et al. Expanded Clinical Evaluation of Lovastatin (EXCEL) study result. I. Efficacy in modifying plasma lipoproteins and adverse event profile in 8245 patients with moderate hypercholesterolemia. Arch Intern Med. 1991;151:43–9. - PubMed
-
- Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of ASCAPS/TexCAPS. JAMA. 1998;279:1615–22. - PubMed
-
- Scandinavian Simvastatin Survival Study Group Randomized trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet. 1994;344:1383–9. - PubMed
-
- The LIPID Study Group Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–57. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous