

When there is too much to do: how practicing physicians prioritize among recommended interventions
- PMID: 15209603
- PMCID: PMC1492380
- DOI: 10.1007/s11606-004-0058-0
When there is too much to do: how practicing physicians prioritize among recommended interventions
Erratum in
- J Gen Intern Med. 2004 Aug;19(8):903
Abstract
Background: Recent evidence suggests that patients are receiving only 50% of recommended processes of care. It is important to understand physician priorities among recommended interventions and how these priorities are influenced both intentionally as well as unintentionally.
Methods: A survey was mailed to all primary care physicians (PCPs) from two VA hospital networks (N= 289), one of which had participated in a broad, evidence-based guideline development effort 8 to 12 months earlier, and all endocrinologists nationwide in the VA (N= 213); response rate, 63% (n= 315). Using the method of paired comparisons, we assessed physician priorities among 11 clinical triggers for interventions in the management of an uncomplicated patient with type 2 diabetes.
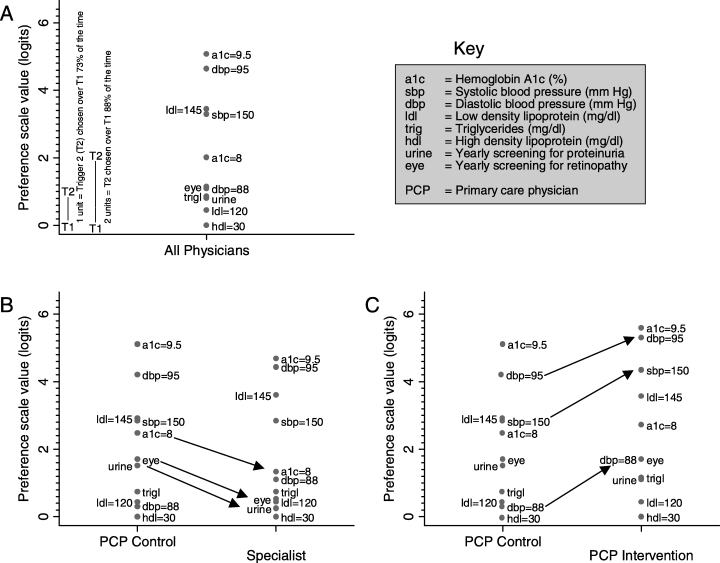
Results: Both PCPs and specialists consistently identified several high-impact clinical triggers for treatment as the highest priority interventions (hemoglobin A1c = 9.5%, diastolic blood pressure [DBP]= 95 mm Hg, low-density lipoprotein = 145 mg/dl). Several low-impact interventions that are commonly used as performance measures also received relatively high ratings. Treatments that have recently been found to be highly beneficial were often rated as being of low importance (e.g., treating when DBP = 88 mm Hg). Almost 80% of PCPs rated tight glycemic control as more important than tight DBP control, in direct contrast to clinical trial evidence. Specialists' ratings followed the same general pattern, but were more consistent with the epidemiological evidence. The PCPs at the sites that participated in the guideline intervention rated blood pressure control significantly higher.
Conclusion: Although several high-priority aspects of diabetes care were clearly identified, there were also notable examples of ratings that were clearly inconsistent with the epidemiological literature. Recommendations based upon more recent evidence were substantially underrated and some guidelines used as performance measures were relatively overrated. These results support the arguments that a more proactive approach is needed to facilitate rapid dissemination of new high-priority findings, and that intervention priority, and not just ease of measurement, should be considered carefully when disseminating guidelines and when selecting performance measures.
Figures
Comment in
-
The many C's of primary care.J Gen Intern Med. 2004 Jun;19(6):708-9. doi: 10.1111/j.1525-1497.2004.40401.x. J Gen Intern Med. 2004. PMID: 15209611 Free PMC article. No abstract available.
References
-
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–45. - PubMed
-
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) JAMA. 2003;289:3095–105. - PubMed
-
- Cabana MD, Rand CS, Becher OJ, Rubin HR. Reasons for pediatrician nonadherence to asthma guidelines. Arch Pediatr Adolesc Med. 2001;155:1057–62. - PubMed
-
- Ruffin MT, Gorenflo DW, Woodman B. Predictors of screening for breast, cervical, colorectal, and prostatic cancer among community-based primary care practices. J Am Board Fam Pract. 2000;13:1–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical