

Neuromonitoring in thyroid surgery: prospective evaluation of intraoperative electrophysiological responses for the prediction of recurrent laryngeal nerve injury
- PMID: 15213612
- PMCID: PMC1356368
- DOI: 10.1097/01.sla.0000132260.34503.02
Neuromonitoring in thyroid surgery: prospective evaluation of intraoperative electrophysiological responses for the prediction of recurrent laryngeal nerve injury
Abstract
Objective: We evaluated the ability of neuromonitoring to predict postoperative outcome in patients undergoing thyroid surgery for different indications.
Summary background data: Neuromonitoring has been advocated to reduce the risk of vocal cord palsy and to predict postoperative vocal cord function.
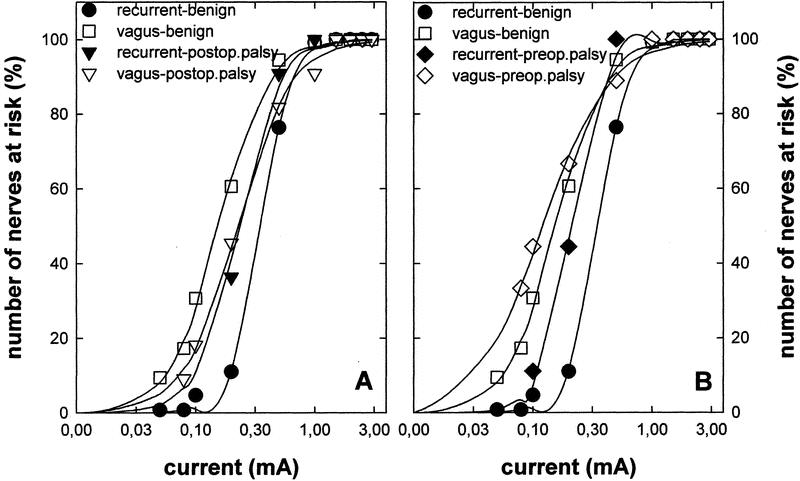
Methods: Three hundred twenty-eight patients (502 nerves at risk) were studied prospectively at a single center. Neuromonitoring was performed with the Neurosign 100 device by transligamental placement of the recording electrode into the vocalis muscles. Cumulative distribution of stimulation thresholds was determined by stepwise decreases in current (1 mA to 0.05 mA) for both the vagus and the recurrent nerve. Patients were grouped according to surgical risk (benign and malignant disease, reoperation for benign and for malignant disease).
Results: If the electrophysiological response was correlated to postoperative vocal cord function, the sensitivity of neuromonitoring was modest (86% in surgery for benign disease) to low (25% in reoperation for malignant disease); the positive predictive value was modest (overall rate 62%) but acceptable (87%) if corrected for technical problems. Specificity and negative predictive values were high (ie, overall >95%). Stimulation thresholds were not augmented in 11 patients, in whom postoperative palsy developed despite normal intraoperative recordings. Similarly, an electrical field response was elicited in 14 of 21 patients with preoperative vocal cord palsy. Electromyographic recordings did not reveal an abnormal amplitude or a decline in nerve conduction velocity.
Conclusions: Neuromonitoring is useful for identifying the recurrent laryngeal nerve, in particular if the anatomic situation is complicated by prior surgery, large tissue masses, aberrant nerve course. However, neuromonitoring does not reliably predict postoperative outcome.
Figures

Comment in
-
Experience counts.Ann Surg. 2004 Jul;240(1):26-7. doi: 10.1097/01.sla.0000130722.43832.f0. Ann Surg. 2004. PMID: 15213614 Free PMC article. No abstract available.
References
-
- Faaborg-Andersen. Electromyographic investigation of intrinsic laryngeal muscles in humans. Acta Physiol Scand. 1957;41(Suppl):140.
-
- Peytz F, Rasmussen H, Buchthal F. Conduction time and velocity in human recurrent laryngeal nerve. Dan Med Bull. 1965;12:125. - PubMed
-
- Flisberg K, Lindholm T. Electrical stimulation of the human recurrent laryngeal nerve during thyroid operation. Acta Otolaryngol (Suppl). 1969;263:63–67. - PubMed
-
- Shedd DP, Burget GC. Identification of the recurrent laryngeal nerve. Arch Surg. 1966;92:861–864. - PubMed
-
- Depisch D. Intraoperative mobility recording of the vocal cord after electrostimulation of the recurrent nerves. Acta Chir Austriaca. 1975;(Suppl 14):1–14.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
