

The Association of Coloproctology of Great Britain and Ireland study of large bowel obstruction caused by colorectal cancer
- PMID: 15213621
- PMCID: PMC1356377
- DOI: 10.1097/01.sla.0000130723.81866.75
The Association of Coloproctology of Great Britain and Ireland study of large bowel obstruction caused by colorectal cancer
Abstract
Background: This study was designed to investigate the early outcomes after surgical treatment of malignant large bowel obstruction (MBO) and to identify risk factors affecting operative mortality.
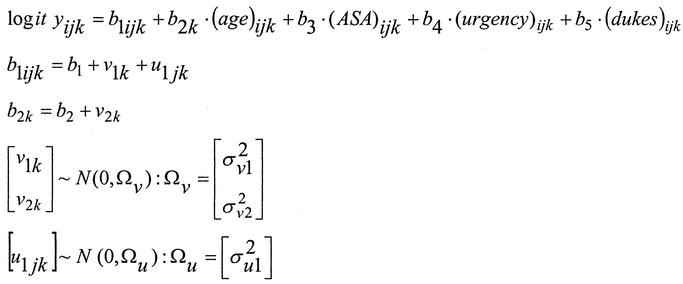
Methods: Data were prospectively collected from 1046 patients with MBO by 294 surgeons in 148 UK hospitals during a 12-month period from April 1998. A predictive model of in-hospital mortality was developed using a 3-level Bayesian logistic regression analysis.
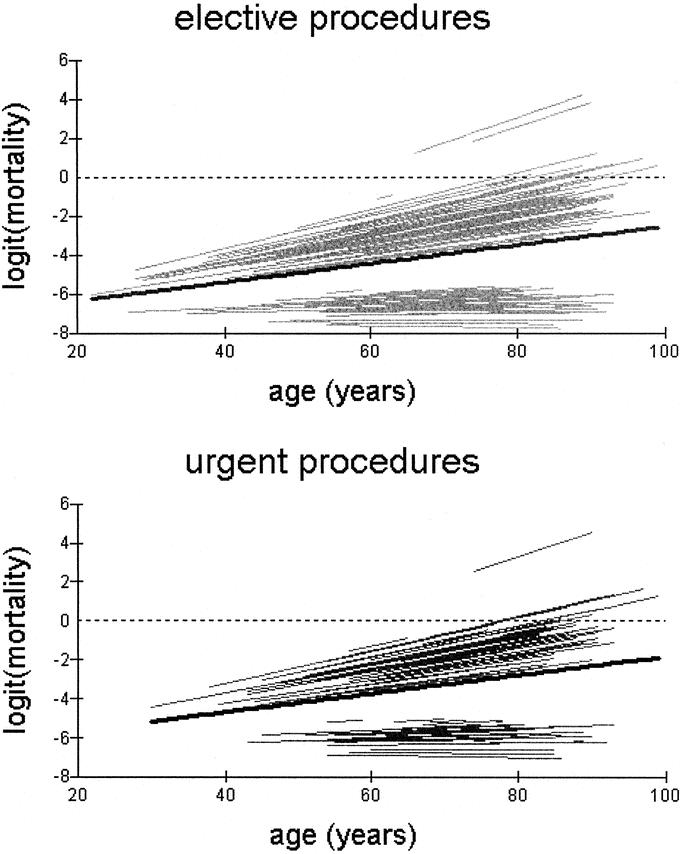
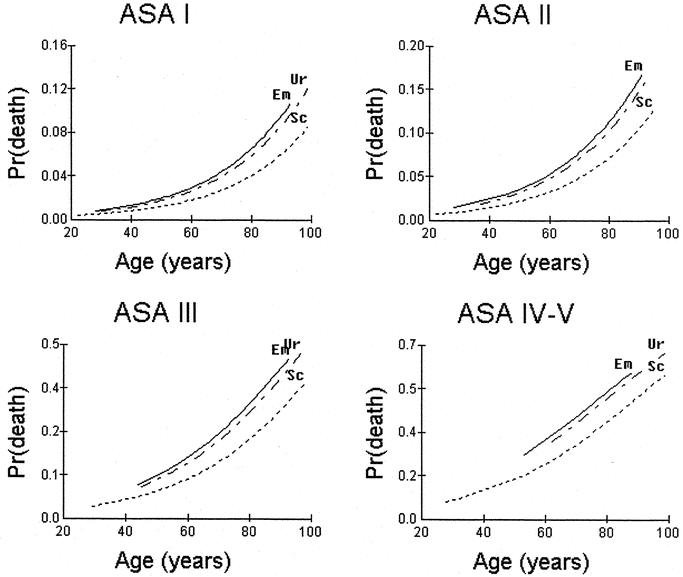
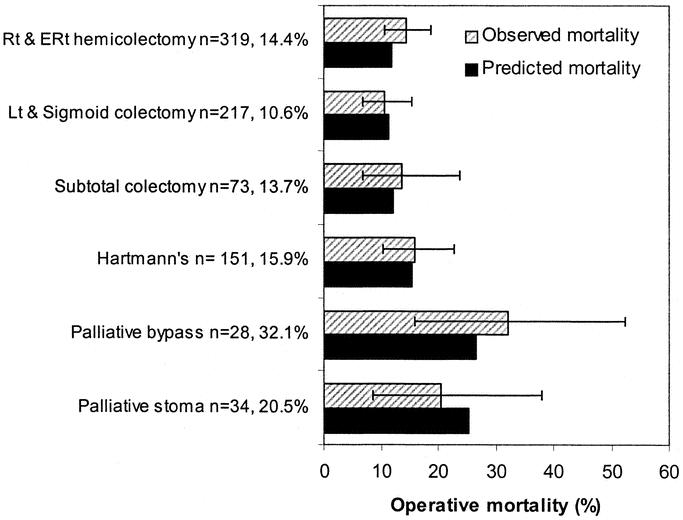
Results: The median age of patients was 73 years (interquartile range 64-80). Of the 989 patients having surgery, 91.7% underwent bowel resection with an overall mortality of 15.7%. The multilevel model used the following independent risk factors to predict mortality: age (odds ratio [OR] 1.85 per 10 year increase), American Society of Anesthesiologists grade (OR for American Society of Anesthesiologists grade I versus II,III,IV-V = 3.3,11.7,22.2), Dukes' staging (OR for Dukes' A versus B,C,D = 2.0, 2.1, 6.0), and mode of surgery (OR for scheduled versus urgent, emergency = 1.6, 2.3). A significant interhospital variability in operative mortality was evident with increasing age (variance = 0.004, SE = 0.001, P < 0.001). No detectable caseload effect was demonstrated between specialist colorectal and other general surgeons.
Conclusions: Using prognostic models, it was possible to develop a risk-stratification index that accurately predicted survival in patients presenting with malignant large bowel obstruction. The methodology and model for risk adjusted survival can set the reference point for more accurate and reliable comparative analysis and be used as an adjunct to the process of informed consent.
Figures
References
-
- Ohman U. Prognosis in patients with obstructing colorectal carcinoma. Am J Surg. 1982;143:742–747. - PubMed
-
- Irvin TT, Greaney MG. The treatment of colonic cancer presenting with intestinal obstruction. Br J Surg. 1977;64:741–744. - PubMed
-
- Phillips RK, Hittinger R, Fry JS, et al. Malignant large bowel obstruction. Br J Surg. 1985;72:296–302. - PubMed
-
- Mulcahy HE, Skelly MM, Husain A, et al. Long-term outcome following curative surgery for malignant large bowel obstruction. Br J Surg. 1996;83:46–50. - PubMed
-
- Wessex Colorectal Cancer Audit. First Report. Wessex Cancer Intelligence Unit, Highcroft, Romsey Road, Winchester SO2 5DH; 1993.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
