

Surgical resection versus percutaneous radiofrequency ablation in the treatment of hepatocellular carcinoma on cirrhotic liver
- PMID: 15213625
- PMCID: PMC1356381
- DOI: 10.1097/01.sla.0000129672.51886.44
Surgical resection versus percutaneous radiofrequency ablation in the treatment of hepatocellular carcinoma on cirrhotic liver
Abstract
Objective: We sought to compare the experience of 2 different surgical units in the treatment of hepatocellular carcinoma (HCC) on cirrhosis with resection or percutaneous radiofrequency ablation (RFA), respectively.
Summary background data: When allowed by the hepatic functional reserve, surgery is the therapy for HCC on cirrhosis; alternative treatments are proposed because of the high tumor recurrence rate after resection. RFA is being widely adopted to treat HCC.
Methods: Over a 4-year period, 79 cirrhotics with HCC underwent resection in 1 surgical unit (group A) and another 79 had RFA at a different unit (group B). Patient selection, operative mortality, hospital stay, and 1- and 3-year overall and disease-free survival were analyzed.
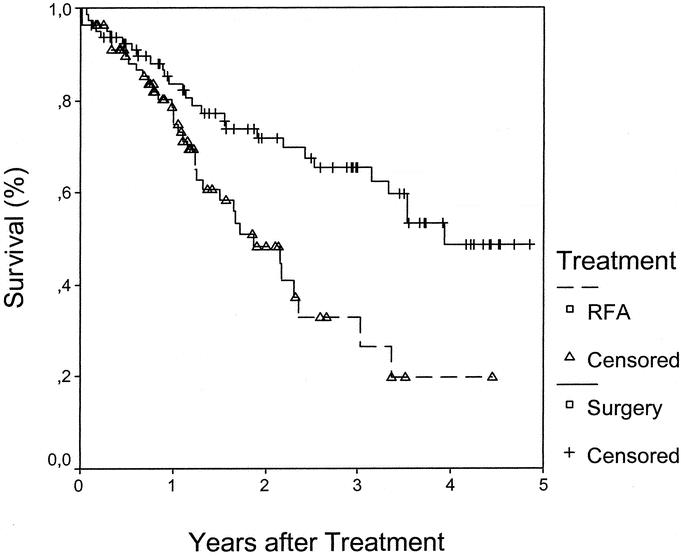
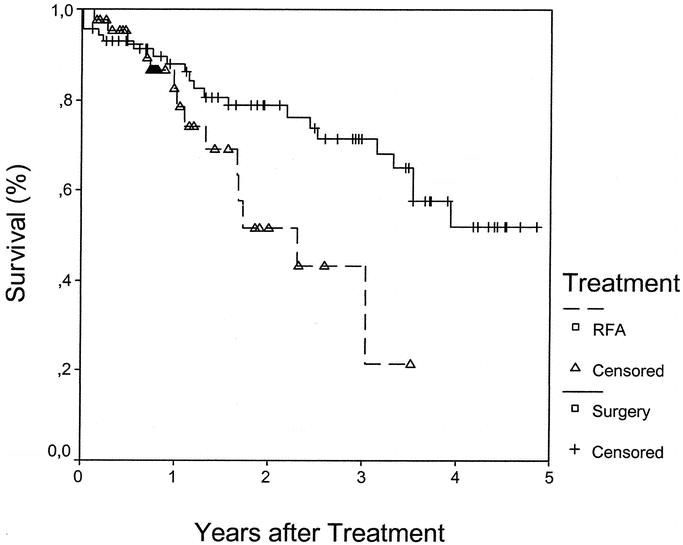
Results: Group A (surgery): mean follow-up was 28.9 +/- 17.9 months; operative mortality was 3.8%, mean hospital stay 9 days; 1- and 3-year survival were, respectively, 83 and 65%. One- and 3-year disease-free survival were 79 and 50%. Group B (RFA): mean follow-up was 15.6 +/- 11.7 months. Mean hospital stay was 1 day (range 1-8). One- and 3-year survival were 78 and 33%; 1- and 3-year disease-free survival were 60 and 20%. Overall and disease-free survival were significantly higher in group A (P = 0.002 and 0.001). The advantage of surgery was more evident for Child-Pugh class A patients and for single tumors of more than 3 cm in diameter. Results were similar in 2 groups for Child-Pugh class B patients
Conclusions: RFA has still to be confirmed as an alternative to surgery for potentially-resectable HCCs.
Figures
References
-
- Martin P. Hepatocellular carcinoma: risk factors and natural history. Liver Transpl Surg. 1998;4(Suppl 1):87–91. - PubMed
-
- Yamamoto J, Kosuge T, Takyama T, et al. Recurrence of hepatocellular carcinoma after surgery. Br J Surg. 1996;83:1219–1222. - PubMed
-
- Wall JW, Marotta PJ. Surgery and transplantation for hepatocellular carcinoma. Liver Transpl. 2000;6:S16–S22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
