

Technical variations in prostatic immunohistochemistry: need for standardisation and stringent quality assurance in PSA and PSAP immunostaining
- PMID: 15220358
- PMCID: PMC1770373
- DOI: 10.1136/jcp.2003.014894
Technical variations in prostatic immunohistochemistry: need for standardisation and stringent quality assurance in PSA and PSAP immunostaining
Abstract
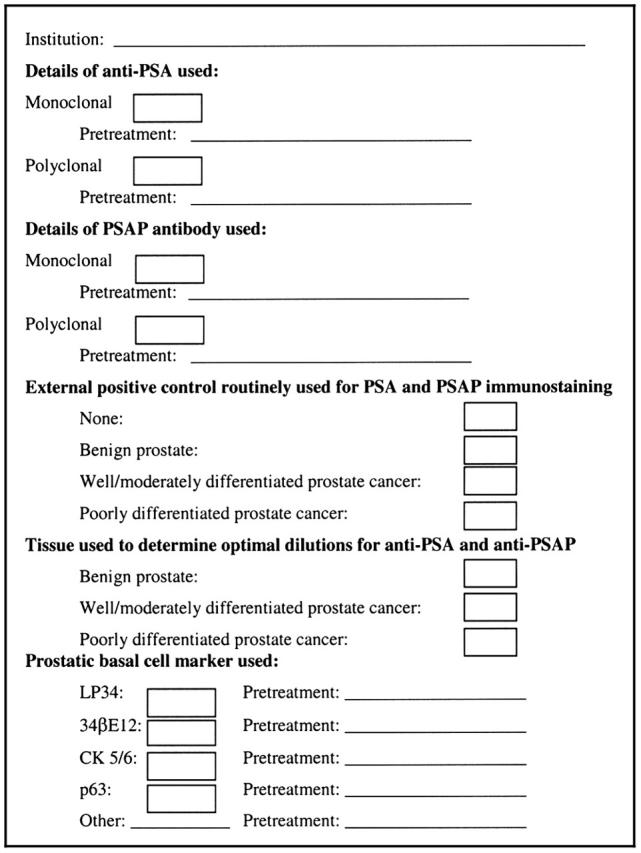
Aims: To assess variations in prostate specific antigen (PSA) and prostate specific acid phosphatase (PSAP) immunohistochemistry with particular reference to the antibody type (monoclonal or polyclonal) and the tissues used for optimising immunostaining conditions and as external positive controls.
Methods: A questionnaire was sent to all laboratories registered with the UK National External Quality Assurance Scheme for immunohistochemistry enquiring about the immunohistochemical methods routinely used for the diagnosis of prostate cancer.
Results: Responses were received from 220 (68%) laboratories. All UK respondents routinely performed PSA immunostaining but PSAP immunostaining was available in only 57% of these laboratories. Monoclonal anti-PSA, polyclonal anti-PSA, monoclonal anti-PSAP, and polyclonal anti-PSAP were used by 40%, 60%, 29%, and 27% of UK respondents, respectively. Benign prostate tissue was most commonly used to determine optimal antibody dilutions and as external quality control for PSA/PSAP, with only 6% and 3% of respondents, respectively, including high grade prostate cancer in the tissues used for these purposes.
Conclusions: The wide variation in the methods used highlights the need for standardisation and more stringent quality assurance of the immunohistochemical staining techniques used for PSA and PSAP. The widespread use of benign prostate tissue to determine optimal antibody dilutions and as an external positive control for PSA and PSAP immunostaining is of particular concern because this approach may result in a method that is not sufficiently sensitive to detect the reduced PSA and PSAP expression associated with high grade prostate cancer.
Figures
References
-
- Wick MR, Mills SE. Consensual interpretive guidelines for diagnostic immunohistochemistry. Am J Surg Pathol 2001;25:1208–10. - PubMed
-
- Seidel T , Balaton AJ, Battifora H. Interpretation and quantification of immunostains. Am J Surg Pathol 2001;25:1204–7. - PubMed
-
- Oliai BR, Kahane H, Epstein JI. A clinicopathologic analysis of urothelial carcinomas diagnosed on prostate needle biopsy. Am J Surg Pathol 2001;25:794–801. - PubMed
-
- Varma M , Morgan M, Jasani MB, et al. Polyclonal anti-PSA is more sensitive but less specific than monoclonal anti-PSA: implications for diagnostic prostatic pathology. Am J Clin Pathol 2002;118:202–7. - PubMed
-
- Goldstein NS. Immunophenotypic characterization of 225 prostate adenocarcinomas with intermediate or high Gleason scores. Am J Clin Pathol 2002;117:471–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous