

Review
doi: 10.1172/JCI22353.
Acute renal failure: definitions, diagnosis, pathogenesis, and therapy
Affiliations
- PMID: 15232604
- PMCID: PMC437979
- DOI: 10.1172/JCI22353
Item in Clipboard
Review
Acute renal failure: definitions, diagnosis, pathogenesis, and therapy
J Clin Invest.
2004 Jul.
Erratum in
- J Clin Invest. 2004 Aug;114(4):598
Abstract
Acute renal failure (ARF), characterized by sudden loss of the ability of the kidneys to excrete wastes, concentrate urine, conserve electrolytes, and maintain fluid balance, is a frequent clinical problem, particularly in the intensive care unit, where it is associated with a mortality of between 50% and 80%. In this review, the epidemiology and pathophysiology of ARF are discussed, including the vascular, tubular, and inflammatory perturbations. The clinical evaluation of ARF and implications for potential future therapies to decrease the high mortality are described.
Figures
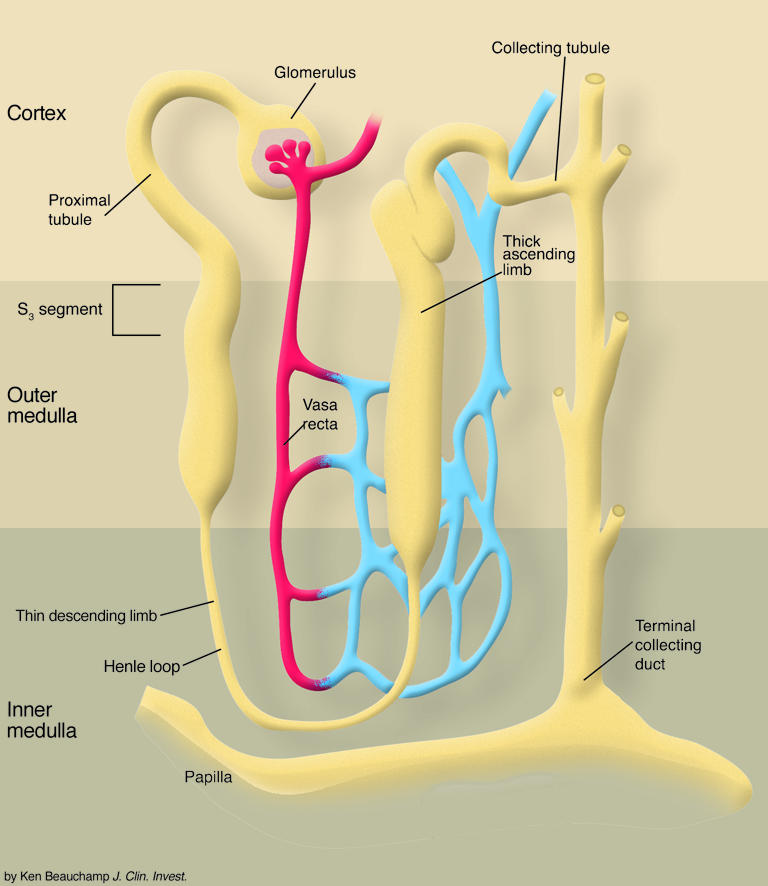
Relative hypoxia in the outer medulla predisposes to ischemic injury in the S3 segment of the proximal tubule. The thick ascending limb is also located in this hypoxic region of the kidney and, depending on tubular reabsorptive demand, may also undergo ischemic injury. The thick ascending limb may, however, be more protected against ischemic injury, because this nephron segment possesses more glycolytic machinery for ATP synthesis than the S3 segment.
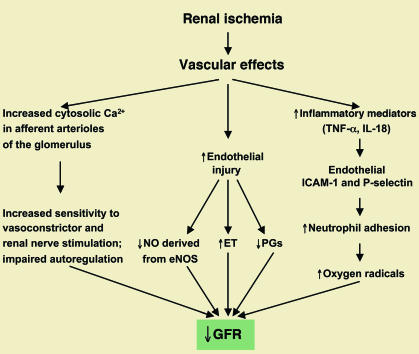
Vascular factors contributing to the pathogenesis of ischemic ARF. ET, endothelin; PG, prostaglandin. Figure modified with permission from the Journal of Nephrology (15).
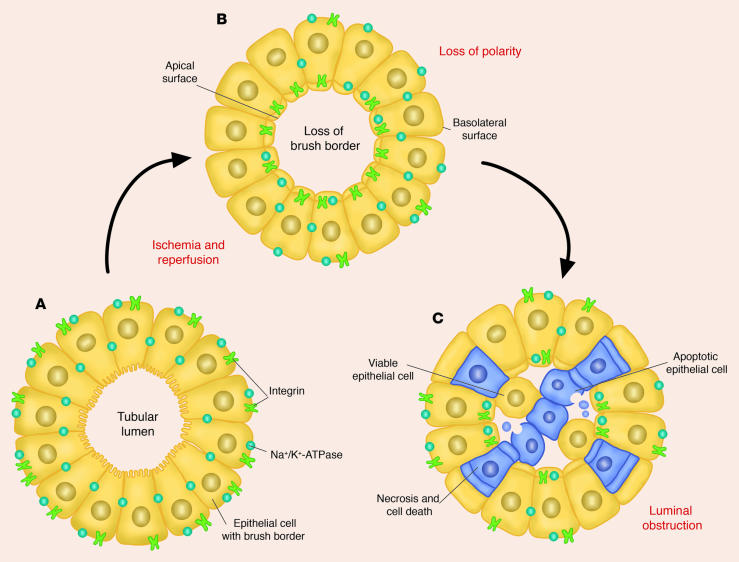
Following ischemia and reperfusion, morphological changes occur in the proximal tubules, including loss of polarity, loss of the brush border, and redistribution of integrins and Na+/K+-ATPase to the apical surface. Calcium and reactive oxygen species may also have a role in these morphological changes, in addition to subsequent cell death resulting from necrosis and apoptosis. Both viable and nonviable cells are shed into the tubular lumen, resulting in the formation of casts and luminal obstruction and contributing to the reduction in the GFR. Figure modified with permission from the New England Journal of Medicine (94).
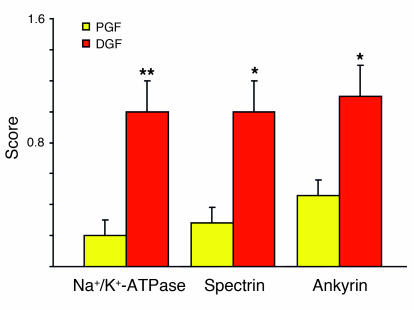
Immunofluorescent staining revealed the cellular location of the actin-binding proteins ankyrin, spectrin, and Na+/K+-ATPase in cadaveric transplanted kidneys with prompt graft function (PGF) and delayed graft function (DGF) (35). The stained sections were examined at ×60–600 magnification using a scanning laser confocal microscope. Scoring was done as follows: 0, continuous staining confined to the basolateral membrane; 0.5, 1.0, and 1.5, interrupted linear staining of basolateral membrane with less than 50%, approximately 50%, and greater than 50% of the staining, respectively, appearing in the cytoplasm. In kidneys with delayed graft function, approximately 50% of the ankyrin, spectrin, and Na+/K+-ATPase was translocated from the basolateral membrane to the cytoplasm, whereas those kidneys with prompt graft function had only minimal translocation of these proteins from the basolateral membrane. *P < 0.01 vs. PGF, **P < 0.05 vs. PGF.
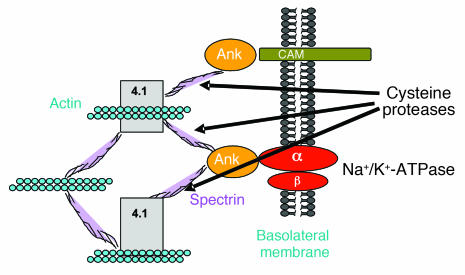
Potential cytoskeletal targets of cysteine proteases during hypoxia/ischemia in proximal tubules. The basolateral membrane of the proximal tubules contains the subunits of Na+/K+-ATPase, which are linked to the actin cytoskeleton by ankyrin and spectrin. This forms a metabolically stable complex. Potential cytoskeletal targets of cysteine proteases during hypoxia/ischemia are shown. Ank, ankyrin; CAM, cell adhesion molecule; 4.1, protein 4.1. Figure reproduced with permission from Taylor & Francis (36).
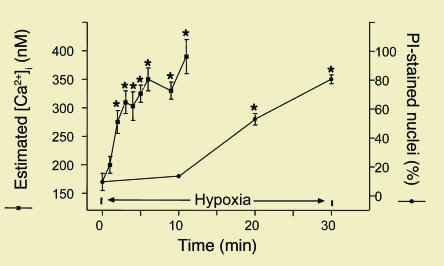
Increased free, intracellular Ca2+ concentration in isolated proximal tubules during hypoxia (measured with the fluorescent Ca2+ indicator Fura-2) precedes cell membrane damage, as assessed by propidium iodide (PI) staining (37). *Significant vs. time 0.
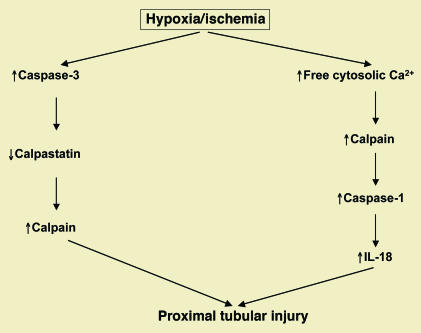
Hypoxic/ischemic proximal tubular necrosis results in activation of cysteine protease pathways involving calpains and both caspase-1 (an inflammatory caspase) and caspase-3 (an executioner caspase involved in apoptosis). Calpain is activated both by increased free cytosolic Ca2+ and decreased calpastatin. Calpain then activates caspase-1, which stimulates the inflammatory cytokine IL-18. The executioner caspase-3 cleaves calpastatin (40).
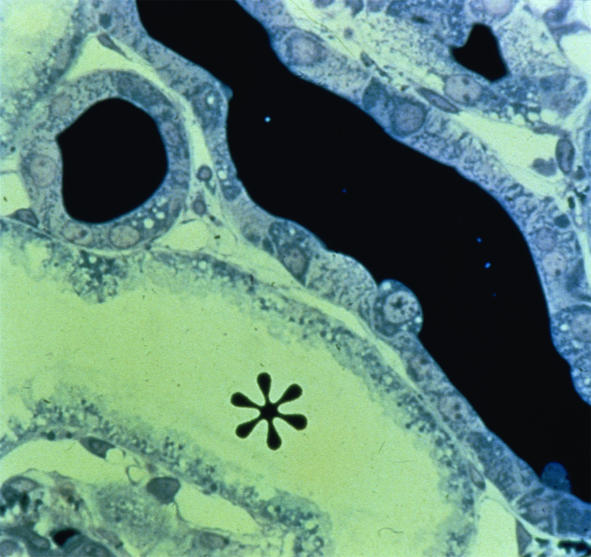
Staining of Tamm-Horsfall protein of casts in renal tubules and dilated tubules in ischemic ARF. The asterisk indicates the tubular lumen. ×100.
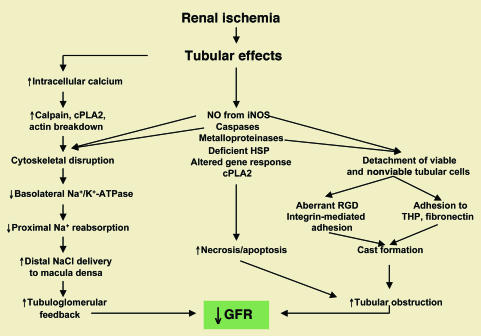
Effects of ischemia on renal tubules in the pathogenesis of ischemic ARF. cPLA2, cytosolic phospholipase A2; HSP, heat shock protein. Figure modified with permission from the Journal of Nephrology (15).
References
-
- Teschan PE, et al. Post-traumatic renal insufficiency in military casualties. I. Clinical characteristics. Am. J. Med. 1955;18:172–186. - PubMed
-
- Smith LH, Jr, et al. Post-traumatic renal insufficiency in military casualties. II. Management, use of an artificial kidney, prognosis. Am. J. Med. 1955;18:187–198. - PubMed
-
- Butkus DE. Post-traumatic acute renal failure in combat casualties: a historical review. Mil. Med. 1984;149:117–124. - PubMed
-
- Whelton A, Donadio JV., Jr Post-traumatic acute renal failure in Vietnam. A comparison with the Korean war experience. Johns Hopkins Med. J. 1969;124:95–105. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
