

A pilot study of antiangiogenic therapy with bevacizumab and thalidomide in patients with metastatic renal cell carcinoma
- PMID: 15235386
- PMCID: PMC2275325
- DOI: 10.1097/00002371-200407000-00001
A pilot study of antiangiogenic therapy with bevacizumab and thalidomide in patients with metastatic renal cell carcinoma
Abstract
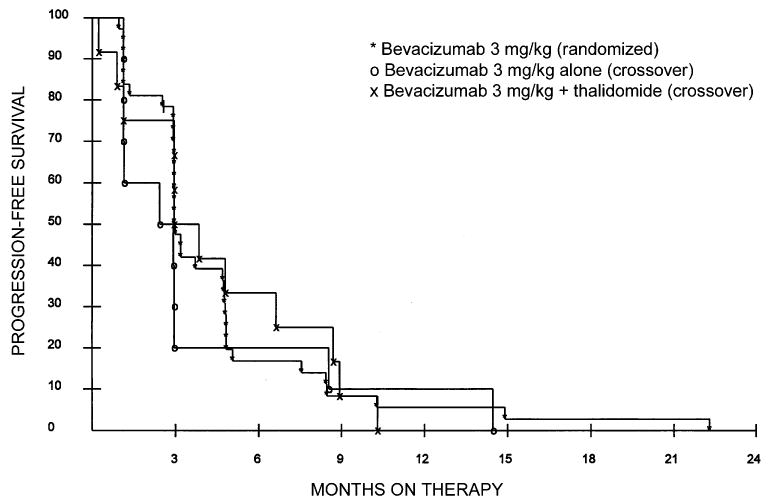
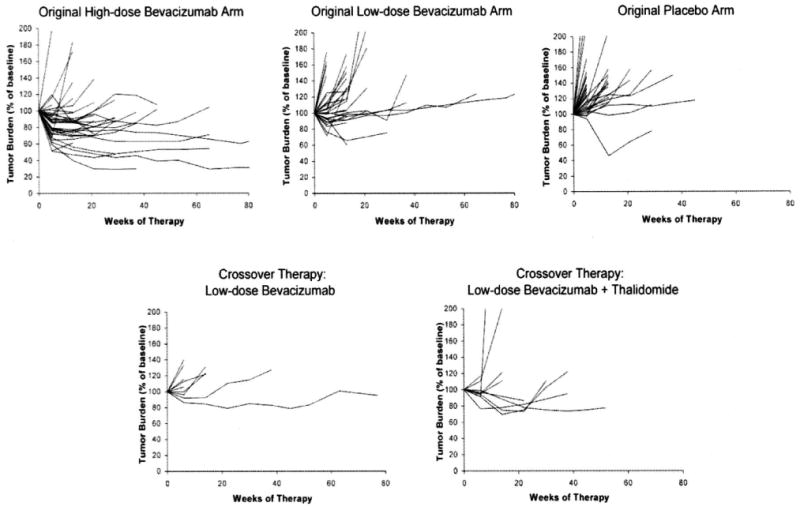
The use of antiangiogenic agents represents a promising strategy for the treatment of patients with metastatic renal cell carcinoma. Objective responses to single-agent thalidomide have been described, and a randomized study showed that bevacizumab (a neutralizing antibody against vascular endothelial growth factor) delayed time to progression of metastatic renal cancer. A pilot study combining these two agents was performed. Sequential cohorts of 10 and 12 patients (crossing over from placebo therapy in the aforementioned randomized bevacizuamab trial) were treated with low-dose bevacizumab alone or bevacizumab plus the maximum tolerated dose of thalidomide as determined by intrapatient escalation. Toxicity, objective responses, and time to progression were the endpoints of this study. Patients tolerated thalidomide and bevacizumab well, with more than 50% of patients escalating to at least 500 mg/d thalidomide. Grades 1 and 2 sensory neuropathy limited thalidomide dose escalation in 3 of 12 patients. The incidence of grades 3 and 4 toxicity was not different between patients treated with bevacizumab alone versus bevacizumab plus thalidomide. There were no objective responses and no difference in progression-free survival between the groups (2.4 months for bevacizumab alone, 3.0 months for bevacizumab plus thalidomide). Combination antiangiogenic therapy with bevacizumab plus thalidomide in patients with renal cell carcinoma is associated with similar toxicity and progression-free survival compared with bevacizumab alone. This study illustrates a clinical trial design for rapidly testing the feasibility and safety of combining antiangiogenic agents, an approach that will be necessary for rapidly evaluating the many potential combinations of antiangiogenic agents.
Figures
References
-
- Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5–26. - PubMed
-
- Motzer RJ, Mazumdar M, Bacik J, et al. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J Clin Oncol. 1999;17:2530–2540. - PubMed
-
- Elson PJ, Witte RS, Trump DL. Prognostic factors for survival in patients with recurrent or metastatic renal cell carcinoma. Cancer Res. 1988;48:7310–7313. - PubMed
-
- Zisman A, Pantuck AJ, Dorey F, et al. Mathematical model to predict individual survival for patients with renal cell carcinoma. J Clin Oncol. 2002;20:1368–1374. - PubMed
-
- Fisher RI, Coltman CA, Jr, Doroshow JH, et al. Metastatic renal cancer treated with interleukin-2 and lymphokine-activated killer cells. A phase II clinical trial. Ann Intern Med. 1988;108:518–523. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
