

Evolution of resistance to drugs in HIV-1-infected patients failing antiretroviral therapy
- PMID: 15238768
- PMCID: PMC2547474
- DOI: 10.1097/01.aids.0000131358.29586.6b
Evolution of resistance to drugs in HIV-1-infected patients failing antiretroviral therapy
Abstract
Background and objective: The optimal time for changing failing antiretroviral therapy (ART) is not known. It involves balancing the risk of exhausting future treatment options against the risk of developing increased drug resistance. The frequency with which new drug-resistance mutations (DRM) developed and their potential consequences in patients continuing unchanged treatment despite persistent viremia were assessed.
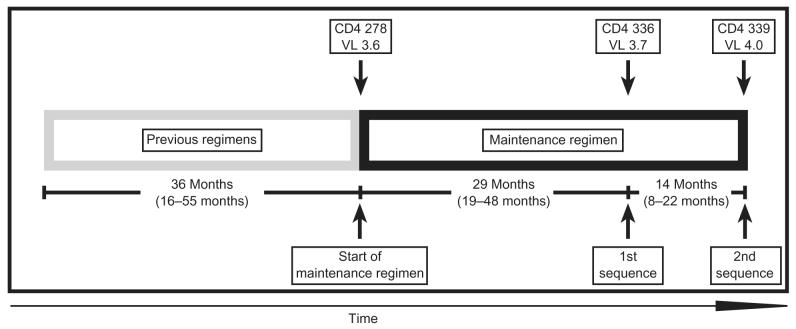
Design: A retrospective study of consecutive sequence samples from 106 patients at one institution with viral load (VL) of more than 400 copies/ml, with no change in ART for more than 2 months despite virologic failure.
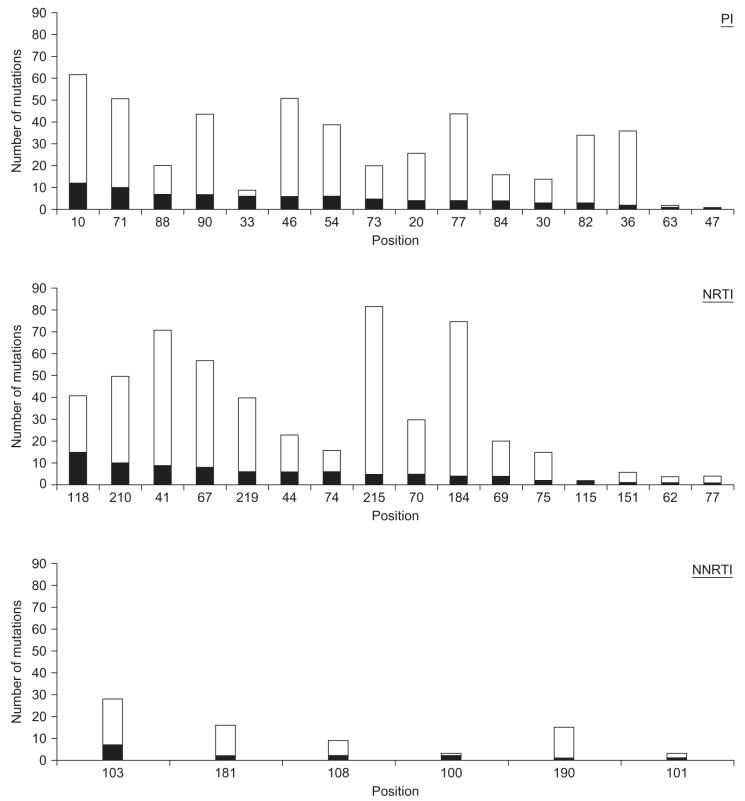
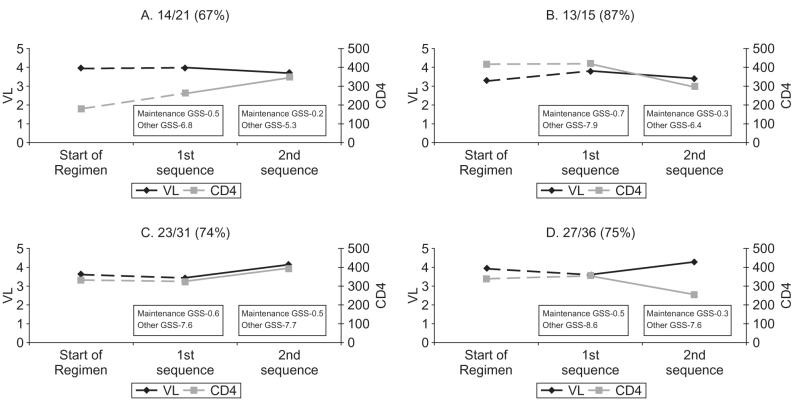
Methods: Two consecutive pol sequences, CD4 cell counts and VL were analyzed to quantify the development of new DRM and to identify changes in immunologic and virologic parameters. Genotypic susceptibility scores (GSS) and viral drug susceptibilities were calculated by a computer program (HIVDB). Poisson log-linear regression models were used to predict the expected number of mutations at the second time point.
Results: : After a median of 14 months of continued ART, 75% (80 of 106) of patients acquired new DRM and were assigned a significantly lower GSS, potentially limiting the success of future ART. The development of new DRM was proportional to the time between the two sequences and inversely proportional to the number of DRM in the first sequence. However, the development of DRM was not associated with significant changes in CD4 or VL counts.
Conclusions: Despite stable levels of CD4 and VL over time, maintaining a failing therapeutic regimen increases drug resistance and may limit future treatment options.
Figures
References
-
- Hirsch MS, Brun-Vezinet F, Clotet B, Conway B, Kuritzkes DR, D’Aquila RT, et al. Antiretroviral drug resistance testing in adults infected with human immunodeficiency virus type 1: 2003 recommendations of an International AIDS Society—USA Panel. Clin Infect Dis. 2003;37:113–128. - PubMed
-
- EuroGuidelines Group for HIV Resistance Clinical and laboratory guidelines for the use of HIV-1 drug resistance testing as part of treatment management: recommendations for the European setting. AIDS. 2001;15:309–320. - PubMed
-
- Parkin NT, Deeks SG, Wrin MT, Yap J, Grant RM, Lee KH, et al. Loss of antiretroviral drug susceptibility at low viral load during early virological failure in treatment-experienced patients. AIDS. 2000;14:2877–2887. - PubMed
-
- Harrigan PR, Hertogs K, Verbiest W, Pauwels R, Larder B, Kemp S, et al. Baseline HIV drug resistance profile predicts response to ritonavir- saquinavir protease inhibitor therapy in a community setting. AIDS. 1999;13:1863–1871. - PubMed
MeSH terms
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
