

Prospective study of a real-time PCR that is highly sensitive, specific, and clinically useful for diagnosis of meningococcal disease in children
- PMID: 15243039
- PMCID: PMC446275
- DOI: 10.1128/JCM.42.7.2919-2925.2004
Prospective study of a real-time PCR that is highly sensitive, specific, and clinically useful for diagnosis of meningococcal disease in children
Abstract
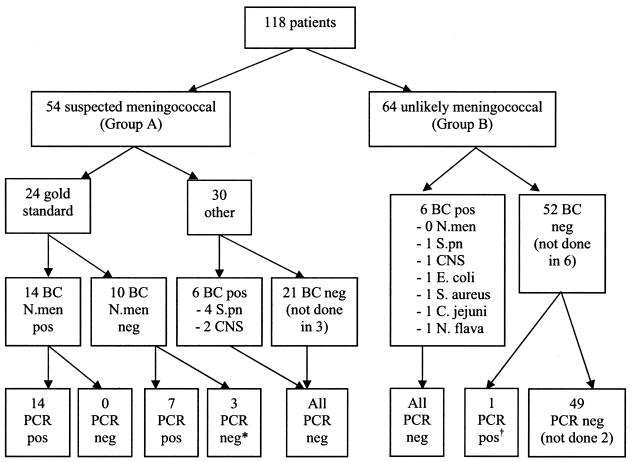
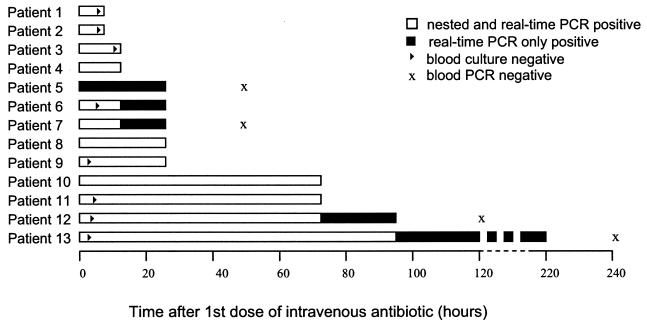
Due to the early administration of antibiotics, meningococcal disease is increasingly difficult to diagnose by culturing. Laboratory studies have shown PCR to be sensitive and specific, but there have been few clinical studies. The objectives of this study were to determine the diagnostic accuracy and clinical usefulness of meningococcal PCR through a prospective comparison of real-time PCR, nested PCR, and standard culturing of blood and cerebrospinal fluid (CSF). The setting was a tertiary-care pediatric hospital in Australia, and the participants were 118 children admitted with possible septicemia or meningitis. The main outcome measures-sensitivity, specificity, and positive and negative predictive values-were compared to a "gold standard " fulfilling clinical and laboratory criteria. For 24 cases of meningococcal disease diagnosed by the gold standard, culturing of blood or CSF was positive for 15 (63%), nested PCR was positive for 21 (88%), and real-time PCR was positive for 23 (96%). The sensitivity, specificity, and positive and negative predictive values of real-time PCR (the most sensitive test) for all specimens were, respectively, 96% (95% confidence interval, 79 to 99%), 100% (95% confidence interval, 96 to 100%), 100% (95% confidence interval, 85 to 100%), and 99% (95% confidence interval, 94 to 100%). Of 54 patients with suspected meningococcal disease at admission, 23 had positive PCR results. Only one PCR specimen was positive in a patient thought unlikely to have meningococcal disease at admission. Blood PCR remained positive for 33% of patients tested at up to 72 h. Real-time PCR has high positive and negative predictive values in this clinical setting, with better confirmation of cases than nested PCR. Targeting patients for PCR based on admission criteria appears to be practical, and the test may remain useful for several days after the start of antibiotic administration.
Figures
Similar articles
-
Dynamics of PCR-based diagnosis in patients with invasive meningococcal disease.Clin Microbiol Infect. 2006 Feb;12(2):137-41. doi: 10.1111/j.1469-0691.2005.01327.x. Clin Microbiol Infect. 2006. PMID: 16441451
-
Polymerase chain reaction for diagnosis and serogrouping of meningococcal disease in children.Diagn Microbiol Infect Dis. 2009 Feb;63(2):148-54. doi: 10.1016/j.diagmicrobio.2008.10.008. Epub 2008 Nov 21. Diagn Microbiol Infect Dis. 2009. PMID: 19026504
-
Diagnosis of meningococcal infection by QPCR: detection and quantification of DNA / Neisseria meningitidis.Rev Med Chir Soc Med Nat Iasi. 2012 Jul-Sep;116(3):888-92. Rev Med Chir Soc Med Nat Iasi. 2012. PMID: 23272547
-
Added value of PCR-testing for confirmation of invasive meningococcal disease in England.J Infect. 2013 Nov;67(5):385-90. doi: 10.1016/j.jinf.2013.06.007. Epub 2013 Jun 22. J Infect. 2013. PMID: 23796865
-
Real-time polymerase chain reaction detection of Neisseria meningitidis in formalin-fixed tissues from sudden deaths.Diagn Microbiol Infect Dis. 2008 Apr;60(4):339-46. doi: 10.1016/j.diagmicrobio.2007.10.014. Epub 2008 Feb 20. Diagn Microbiol Infect Dis. 2008. PMID: 18068935
Cited by
-
Neurologic Manifestations of the World Health Organization's List of Pandemic and Epidemic Diseases.Front Neurol. 2021 Feb 22;12:634827. doi: 10.3389/fneur.2021.634827. eCollection 2021. Front Neurol. 2021. PMID: 33692745 Free PMC article. Review.
-
Real-time polymerase chain reaction for the rapid detection of group B streptococcal colonization in neonates.Pediatrics. 2006 Jul;118(1):14-22. doi: 10.1542/peds.2005-1594. Pediatrics. 2006. PMID: 16818544 Free PMC article.
-
Diagnosis of bacterial meningitis in Ghana: Polymerase chain reaction versus latex agglutination methods.PLoS One. 2019 Jan 17;14(1):e0210812. doi: 10.1371/journal.pone.0210812. eCollection 2019. PLoS One. 2019. PMID: 30653582 Free PMC article.
-
Fatal meningococcal meningitis in a 2-year-old child: A case report.World J Clin Cases. 2019 Mar 6;7(5):636-641. doi: 10.12998/wjcc.v7.i5.636. World J Clin Cases. 2019. PMID: 30863763 Free PMC article.
-
Diagnostic Accuracy of Cerebrospinal Fluid Multiplex Polymerase Chain Reaction Panel Testing in Patients With Suspected Central Nervous System Infections: A Multi-Center Study in the United Arab Emirates.Cureus. 2024 Jan 8;16(1):e51906. doi: 10.7759/cureus.51906. eCollection 2024 Jan. Cureus. 2024. PMID: 38333447 Free PMC article.
References
-
- al Wali, W., and C. Hughes. 1998. Urine antigen detection can be quicker than PCR in the diagnosis of meningococcal disease. J. Hosp. Infect. 40:326-328. - PubMed
-
- Anonymous. 2001. Guidelines for the early clinical and public health management of meningococcal disease in Australia, p. 8. Commonwealth Department of Health and Aged Care, Canberra, Australia.
-
- Bohr, V., N. Rasmussen, B. Hansen, H. Kjersem, O. Jessen, N. Johnsen, and H. S. Kristensen. 1983. 875 cases of bacterial meningitis: diagnostic procedures and the impact of preadmission antibiotic therapy. Part III of a three-part series. J. Infect. 7:193-202. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
