

Measurement of vitamin D levels in inflammatory bowel disease patients reveals a subset of Crohn's disease patients with elevated 1,25-dihydroxyvitamin D and low bone mineral density
- PMID: 15247180
- PMCID: PMC1774134
- DOI: 10.1136/gut.2003.036657
Measurement of vitamin D levels in inflammatory bowel disease patients reveals a subset of Crohn's disease patients with elevated 1,25-dihydroxyvitamin D and low bone mineral density
Abstract
Objectives: Many patients with Crohn's disease (CD) have low bone mineral density (BMD) that may not be solely attributable to glucocorticoid use. We hypothesised that low BMD in patients with CD is associated with elevated circulating levels of the active form of vitamin D, 1,25-dihydroxyvitamin D (1,25(OH)(2)D). We further hypothesised that this was secondary to increased synthesis of 1,25(OH)(2)D by inflammatory cells in the intestine. The aim of this study was to examine the relationship between 1,25(OH)(2)D levels and BMD in patients with CD.
Methods: An IRB approved retrospective review of medical records from patients with CD (n = 138) or ulcerative colitis (UC, n = 29). Measurements of vitamin D metabolites and immunoreactive parathyroid hormone (iPTH) were carried out. BMD results were available for 88 CD and 20 UC patients. Immunohistochemistry or real time reverse transcription-polymerase chain reaction (RT-PCR) for the enzyme 1alpha-hydroxylase was performed on colonic biopsies from patients with CD (14) or UC (12) and normal colons (4).
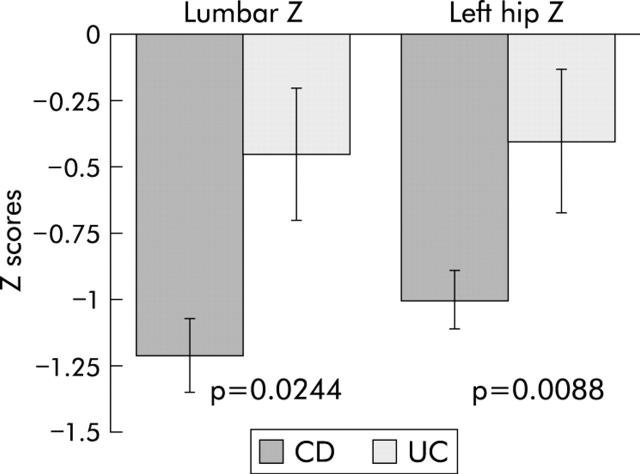
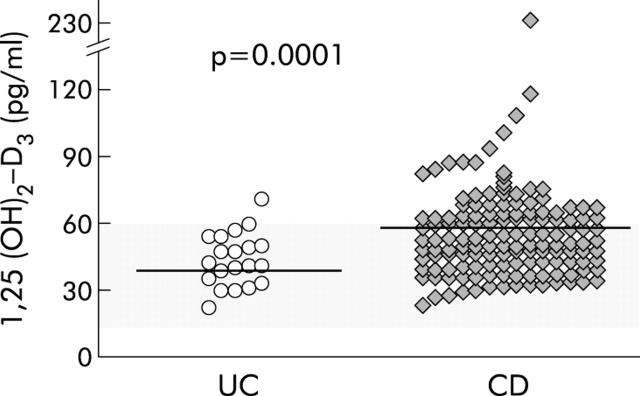
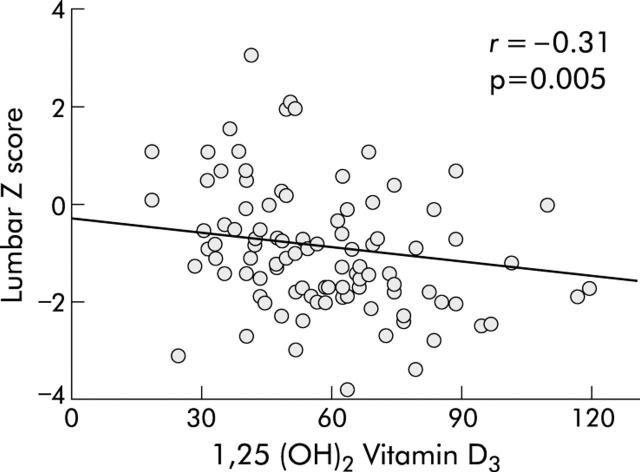
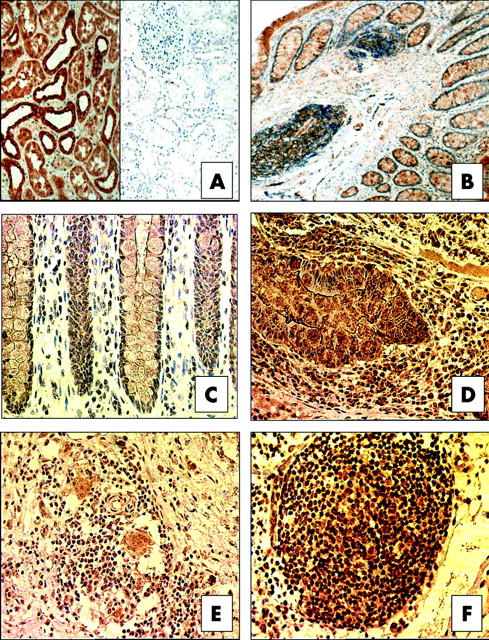
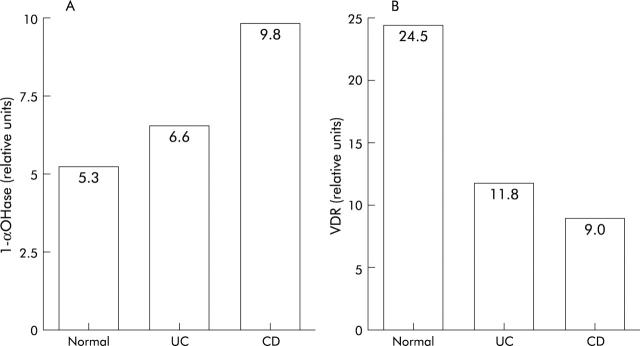
Results: Inappropriately high levels of serum 1,25(OH)(2)D (>60 pg/ml) were observed in 42% of patients with CD compared with only 7% in UC, despite no differences in mean iPTH. Serum 1,25(OH)(2)D levels were higher in CD (57 pg/ml) versus UC (41 pg/ml) (p = 0.0001). In patients with CD, there was a negative correlation between 1,25(OH)(2)D levels and lumbar BMD (r = -0.301, p = 0.005) independent of therapeutic glucocorticoid use. 1,25(OH)(2)D levels also correlated with CD activity. Lastly, immunohistochemistry and RT-PCR demonstrated increased expression of intestinal 1alpha-hydroxylase in patients with CD.
Conclusions: These data demonstrate that elevated 1,25(OH)(2)D is more common in CD than previously appreciated and is independently associated with low bone mineral density. The source of the active vitamin D may be the inflamed intestine. Treatment of the underlying inflammation may improve metabolic bone disease in this subgroup of patients.
Figures
Similar articles
-
Vitamin D Status and Bone Mineral Density in Children with Inflammatory Bowel Disease Compared to Those with Functional Abdominal Pain.J Korean Med Sci. 2017 Jun;32(6):961-967. doi: 10.3346/jkms.2017.32.6.961. J Korean Med Sci. 2017. PMID: 28480654 Free PMC article.
-
Vitamin D levels and bone metabolism in Chinese adult patients with inflammatory bowel disease.J Dig Dis. 2014 Mar;15(3):116-23. doi: 10.1111/1751-2980.12118. J Dig Dis. 2014. PMID: 24354597
-
Vitamin D receptor (VDR) TaqI polymorphism, vitamin D and bone mineral density in patients with inflammatory bowel diseases.Adv Clin Exp Med. 2019 Jul;28(7):955-960. doi: 10.17219/acem/97376. Adv Clin Exp Med. 2019. PMID: 30929318
-
1alpha(OH)D3 One-alpha-hydroxy-cholecalciferol--an active vitamin D analog. Clinical studies on prophylaxis and treatment of secondary hyperparathyroidism in uremic patients on chronic dialysis.Dan Med Bull. 2008 Nov;55(4):186-210. Dan Med Bull. 2008. PMID: 19232159 Review.
-
Vitamin D and Crohn's disease in the adult patient: a review.JPEN J Parenter Enteral Nutr. 2014 May;38(4):438-58. doi: 10.1177/0148607113506013. Epub 2013 Oct 23. JPEN J Parenter Enteral Nutr. 2014. PMID: 24154811 Review.
Cited by
-
Bone Metabolism Alteration in Patients with Inflammatory Bowel Disease.J Clin Med. 2022 Jul 16;11(14):4138. doi: 10.3390/jcm11144138. J Clin Med. 2022. PMID: 35887903 Free PMC article.
-
Transcriptional activity of vitamin D receptor in human periodontal ligament cells is diminished under inflammatory conditions.J Periodontol. 2021 Jan;92(1):137-148. doi: 10.1002/JPER.19-0541. Epub 2020 Jun 21. J Periodontol. 2021. PMID: 32474936 Free PMC article.
-
Lactic Acid Bacteria Isolated From Korean Kimchi Activate the Vitamin D Receptor-autophagy Signaling Pathways.Inflamm Bowel Dis. 2020 Jul 17;26(8):1199-1211. doi: 10.1093/ibd/izaa049. Inflamm Bowel Dis. 2020. PMID: 32170938 Free PMC article.
-
Immunostimulation in the era of the metagenome.Cell Mol Immunol. 2011 May;8(3):213-25. doi: 10.1038/cmi.2010.77. Epub 2011 Jan 31. Cell Mol Immunol. 2011. PMID: 21278764 Free PMC article. Review.
-
Impact of Paneth Cell Autophagy on Inflammatory Bowel Disease.Front Immunol. 2018 Apr 5;9:693. doi: 10.3389/fimmu.2018.00693. eCollection 2018. Front Immunol. 2018. PMID: 29675025 Free PMC article. Review.
References
-
- Adachi JD, Rostom A. Metabolic bone disease in adults with inflammatory bowel disease. Inflamm Bowel Dis 1999;5:200–11. - PubMed
-
- Clements D , Motley RJ, Evans WD, et al. Longitudinal study of cortical bone loss in patients with inflammatory bowel disease. Scand J Gastroenterol 1992;27:1055–60. - PubMed
-
- Motley RJ, Clements D, Evans WD, et al. A four-year longitudinal study of bone loss in patients with inflammatory bowel disease. Bone Miner 1993;23:95–104. - PubMed
-
- Valentine JF, Sninsky CA. Prevention and treatment of osteoporosis in patients with inflammatory bowel disease. Am J Gastroenterol 1999;94:878–83. - PubMed
-
- Bertolini DR, Nedwin GE, Bringman TS, et al. Stimulation of bone resorption and inhibition of bone formation in vitro by human tumour necrosis factors. Nature 1986;319:516–18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical