

Review
doi: 10.1136/gut.2003.025460.
Endoscopic antireflux procedures
Affiliations
- PMID: 15247192
- PMCID: PMC1774149
- DOI: 10.1136/gut.2003.025460
Item in Clipboard
Review
Endoscopic antireflux procedures
Gut.
2004 Aug.
No abstract available
Figures
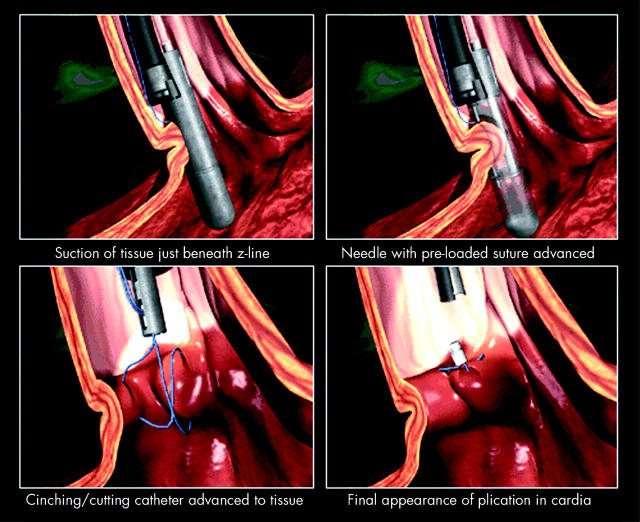
Schematic overview of the Endocinch procedure (reproduced with permission from Bard).

The Wilson-Cook endoscopic suturing system. The device is attached to the endoscope through an external accessory channel. The capsule contains two needles so that the creation of one plication is possible without removal of the suturing device out of the patient (reproduced with permission from Wilson-Cook).
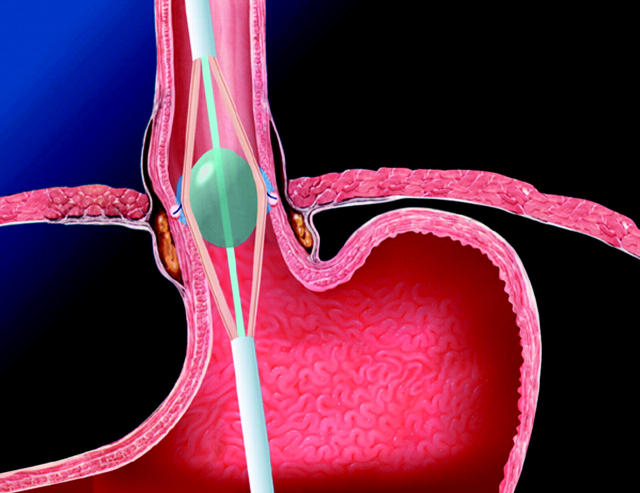
Overview of the Stretta catheter placed at the gastro-oesophageal junction for radiofrequency energy delivery (reproduced with permission from Curon).
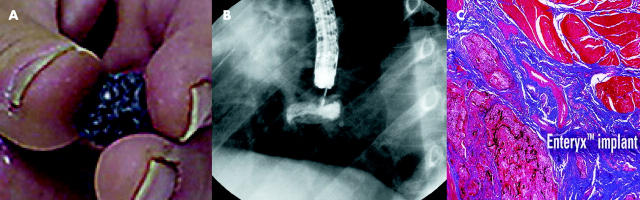
Overview of the Enteryx procedure. (A) Foamy particles of biopolymer after solidification in water. (B) Ring-like aspect of biopolymer after injection at the lower oesophageal sphincter. (C) Histological feature of the reaction induced by biopolymer injection (reproduced with permission from Boston Scientific).
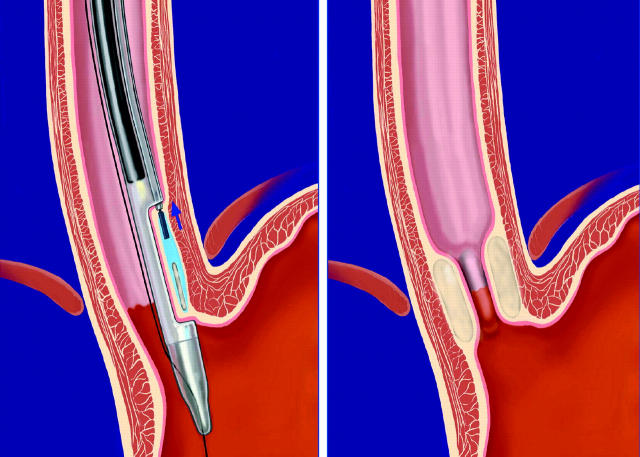
Schematic overview of the Gatekeeper system (reproduced with permission from Medtronic).
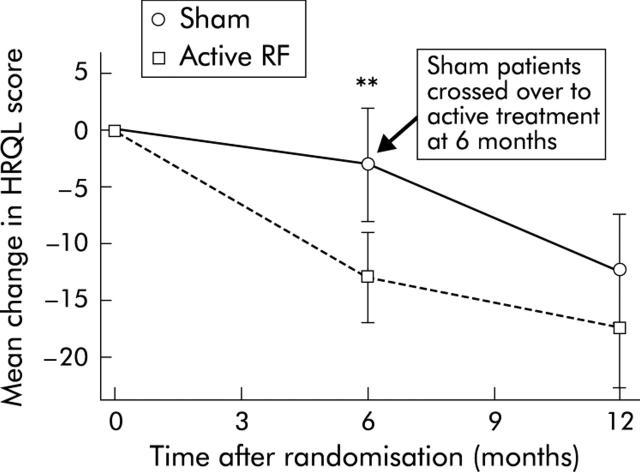
Change in mean gastro-oesophageal reflux disease quality of life (HRQRL score). Sham patients were crossed over to active treatment at the six month evaluation. **Significant difference between active and sham treatment at six months (p = 0.003). RF, radiofrequency (reproduced with permission from the editor of Gastroenterology).
References
-
- Lagergren J , Bergström R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for oesophageal adenocarcinoma. N Engl J Med 1999;340:825–31. - PubMed
-
- Locke GR III, Talley NG, Fett SL, et al. Prevalence and clinical spectrum of gastroesophageal reflux: a population-bases study in Olmsted County. Gastroenterology 1997;112:1448–56. - PubMed
-
- Tytgat GN. Shortcomings of the first-generation proton pomp inhibitors. Eur J Gastroenterol Hepatol 2001;13 (suppl 1) :S29–33. - PubMed
-
- Bardhan KD. The role of the proton pomp inhibitors in the treatment of gastroesophageal reflux disease. Aliment Pharmacol Ther 1999;9 (suppl 1) :15–25. - PubMed
-
- Pegini PL, Katz PO, Castell DO. Ranitidine controls nocturnal gastric acid breakthrough on omeprazole: a controlled study in normal subjects. Gastroenterology 1998;155:1335–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical