

Randomized comparison of the effects of the vitamin D3 adequate intake versus 100 mcg (4000 IU) per day on biochemical responses and the wellbeing of patients
- PMID: 15260882
- PMCID: PMC506781
- DOI: 10.1186/1475-2891-3-8
Randomized comparison of the effects of the vitamin D3 adequate intake versus 100 mcg (4000 IU) per day on biochemical responses and the wellbeing of patients
Abstract
Background: For adults, vitamin D intake of 100 mcg (4000 IU)/day is physiologic and safe. The adequate intake (AI) for older adults is 15 mcg (600 IU)/day, but there has been no report focusing on use of this dose.
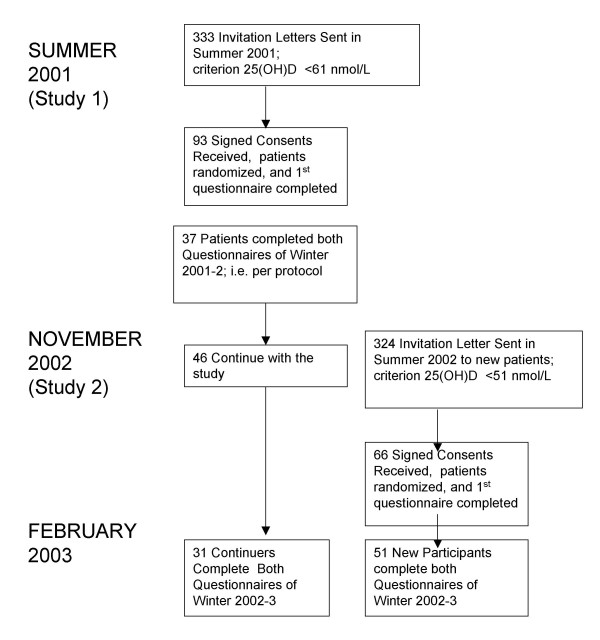
Methods: We compared effects of these doses on biochemical responses and sense of wellbeing in a blinded, randomized trial. In Study 1, 64 outpatients (recruited if summer 2001 25(OH)D <61 nmol/L) were given 15 or 100 mcg/day vitamin D in December 2001. Biochemical responses were followed at subsequent visits that were part of clinical care; 37 patients completed a wellbeing questionnaire in December 2001 and February 2002. Subjects for Study 2 were recruited if their 25(OH)D was <51 nmol/L in summer 2001. 66 outpatients were given vitamin D; 51 completed a wellbeing questionnaire in both December 2002 and February 2003.
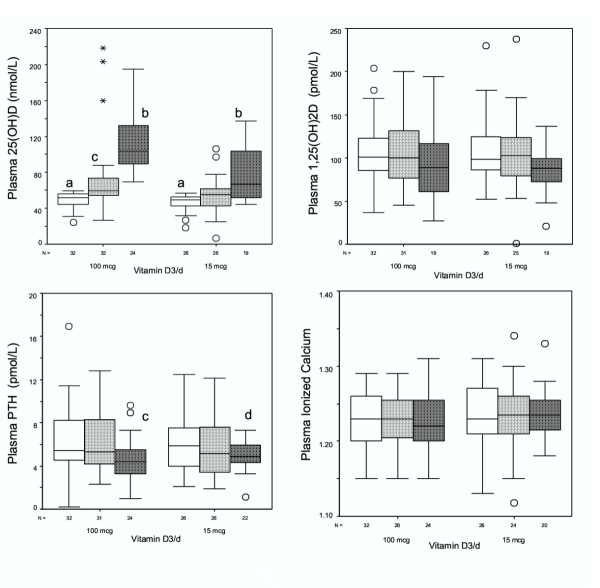
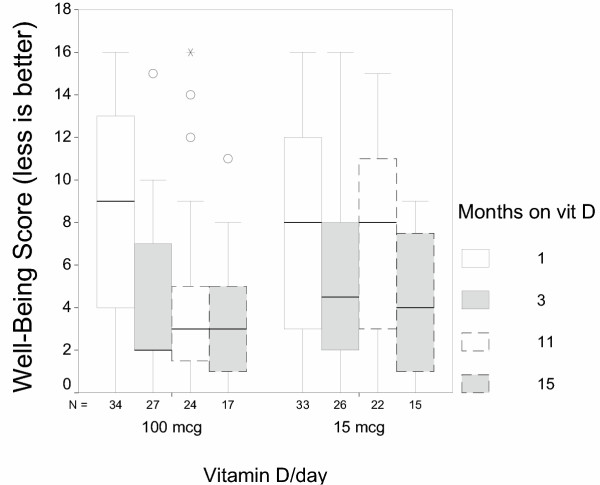
Results: In Study 1, basal summer 25-hydroxyvitamin D [25(OH)D] averaged 48 +/- 9 (SD) nmol/L. Supplementation for more than 6 months produced mean 25(OH)D levels of 79 +/- 30 nmol/L for the 15 mcg/day group, and 112 +/- 41 nmol/L for the 100 mcg/day group. Both doses lowered plasma parathyroid hormone with no effect on plasma calcium. Between December and February, wellbeing score improved more for the 100-mcg/day group than for the lower-dosed group (1-tail Mann-Whitney p = 0.036). In Study 2, 25(OH)D averaged 39 +/- 9 nmol/L, and winter wellbeing scores improved with both doses of vitamin D (two-tail p < 0.001).
Conclusion: The highest AI for vitamin D brought summertime 25(OH)D to >40 nmol/L, lowered PTH, and its use was associated with improved wellbeing. The 100 mcg/day dose produced greater responses. Since it was ethically necessary to provide a meaningful dose of vitamin D to these insufficient patients, we cannot rule out a placebo wellbeing response, particularly for those on the lower dose. This work confirms the safety and efficacy of both 15 and 100 mcg/day vitamin D3 in patients who needed additional vitamin D.
Figures
References
-
- Dawson-Hughes B, Heaney R, Lips P, Meunier P, Vieth R. Vitamin D Round Table. In: Dawson-HughesB, HeaneyR and BurckhardtP, editor. Nutritional Aspects of Osteoporosis. In press. New York, Academic Press; 2004.
-
- Yates AA. Process and development of dietary reference intakes: basis, need, and application of recommended dietary allowances. Nutr Rev. 1998;56:S5–S9. - PubMed
-
- Intakes. Standing Committee on the Scientific Evaluation of Dietary Reference. Dietary reference intakes: calcium, phosphorus, magnesium, vitamin D, and fluoride. National Academy Press; 1997.
-
- Vieth R, Chan PC, MacFarlane GD. Efficacy and safety of vitamin D(3) intake exceeding the lowest observed adverse effect level. Am J Clin Nutr. 2001;73:288–294. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
